

Compliance With a Comprehensive Antibiotic Protocol Improves Infection Incidence in Pediatric Spine Surgery
- PMID: 27280896
- PMCID: PMC5145789
- DOI: 10.1097/BPO.0000000000000812
Compliance With a Comprehensive Antibiotic Protocol Improves Infection Incidence in Pediatric Spine Surgery
Abstract
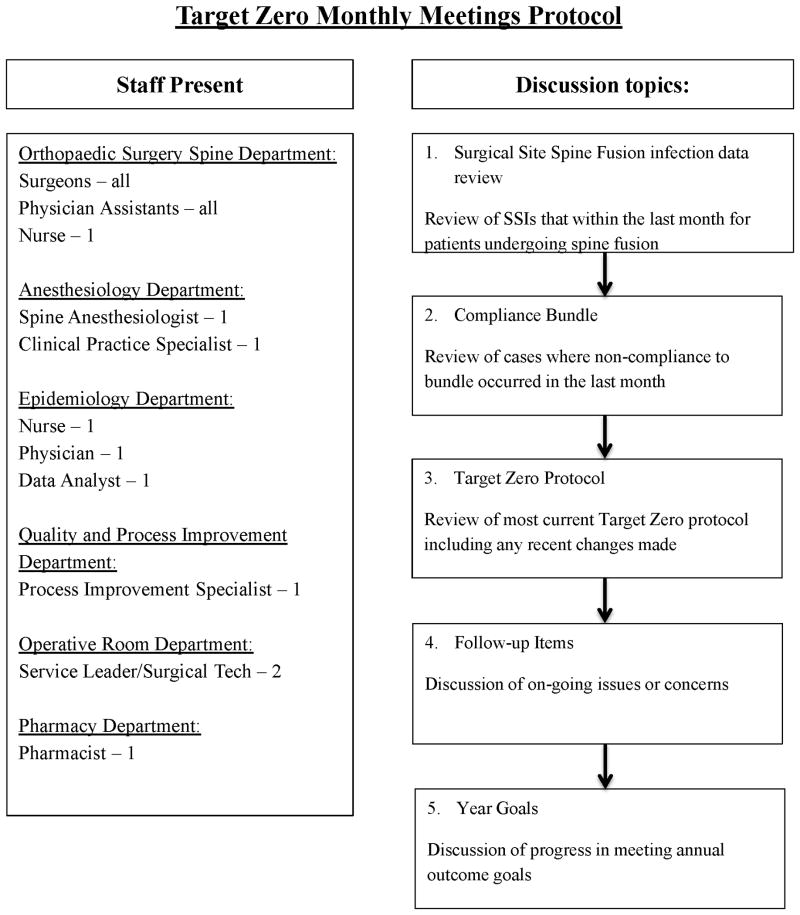
Background: A multidisciplinary task force, designated Target Zero, has developed protocols for prevention of surgical site infection (SSI) for spine surgery at our institution. The purpose of this study was to evaluate how compliance with an antibiotic bundle impacts infection incidences in pediatric spine surgery.
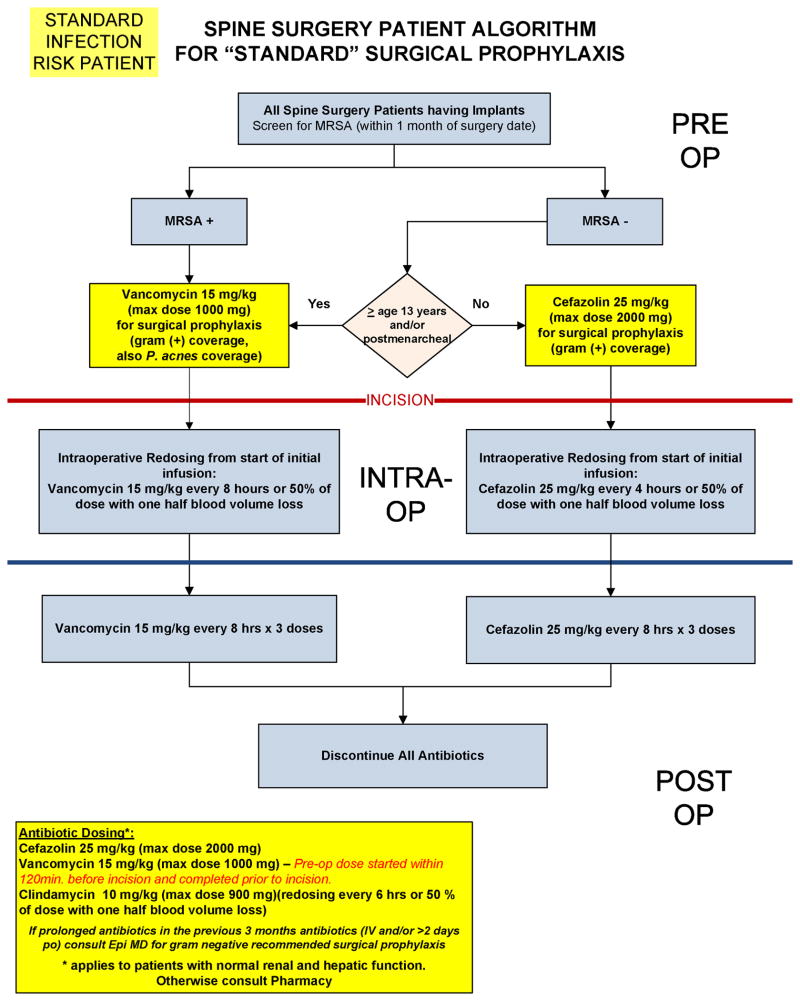
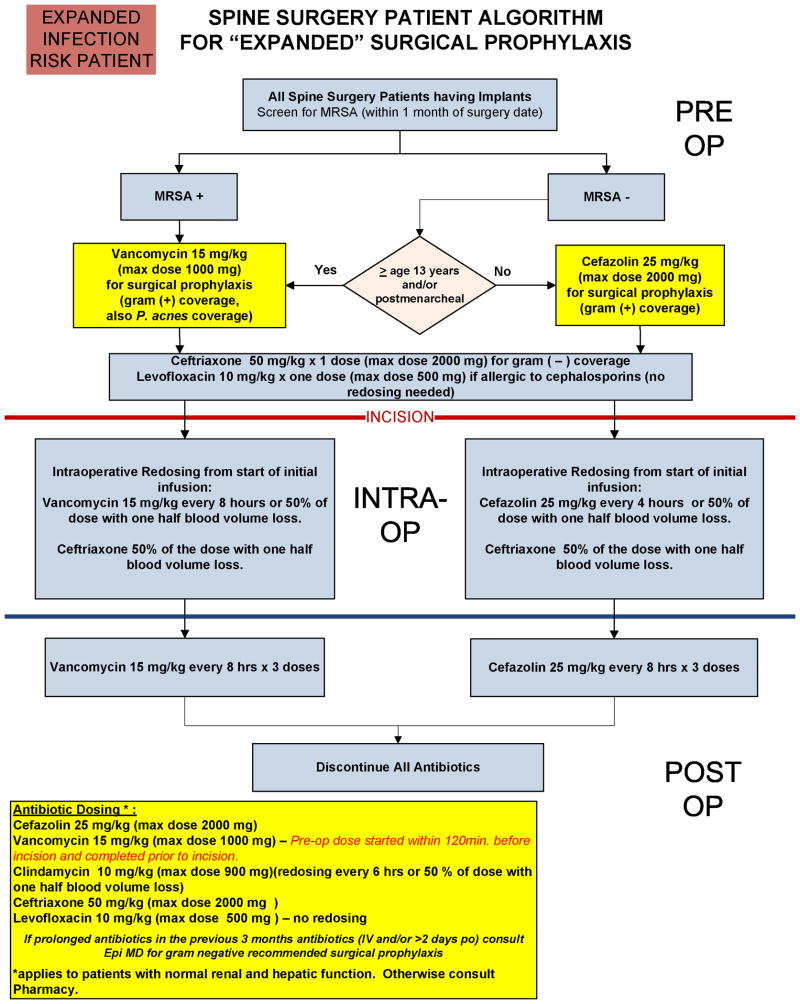
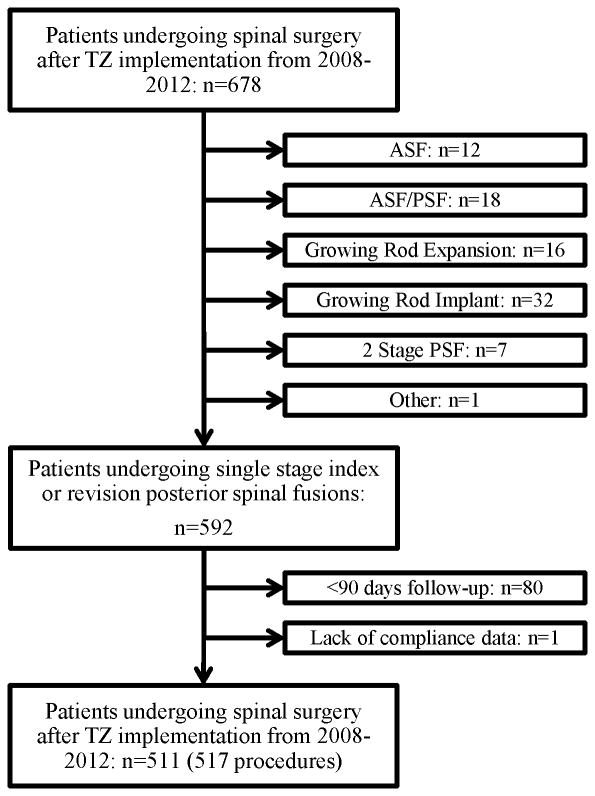
Methods: After institutional review board approval, a consecutive series of 511 patients (517 procedures) who underwent primary spine procedures from 2008 to 2012 were retrospectively reviewed to identify patients who developed SSI. Patients were followed for a minimum of 90 days postoperatively. Compliance data were collected prospectively in 511 consecutive patients and a total of 517 procedures. Three criteria were required for antibiotic bundle compliance: appropriate antibiotics completely administered within 1 hour before incision, antibiotics appropriately redosed intraoperatively for blood loss and time, and antibiotics discontinued within 24 hours postoperatively. A multivariable logistic regression analysis was used to test the association between compliance and the development of an infection.
Results: Overall antibiotic bundle compliance rate was 85%. After adjusting for risk category, estimated blood loss, and study year, the likelihood of an infection was increased in the noncompliant group compared with the compliant group (adjusted odds ratio: 3.0, 95% CI, 0.96-9.47, P=0.0587). When expressed as the number needed to treat, strict adherence to antibiotic bundle compliance prevented 1 SSI within 90 days of surgery for every 26 patients treated with the antibiotic bundle. Reasons for noncompliance included failure to infuse preoperative antibiotics 1 hour before incision (10.3%), failure to redose antibiotics intraoperatively based on time or blood loss (5.5%), and failure to discontinue antibiotics within 24 hours postoperatively (1.9%).
Conclusions: Compliance with a comprehensive antibiotic protocol can lead to meaningful reductions in SSI incidences in pediatric spine surgery. Institutions should focus on improving compliance with prophylactic antibiotic protocols to decrease SSI in pediatric spine surgery.
Level of evidence: Level III-retrospective cohort study.
Conflict of interest statement
Figures
References
-
- Cahill PJ, et al. Infection after spinal fusion for pediatric spinal deformity: thirty years of experience at a single institution. Spine (Phila Pa 1976) 2010;35(12):1211–7. - PubMed
-
- Ho C, et al. Management of infection after instrumented posterior spine fusion in pediatric scoliosis. Spine (Phila Pa 1976) 2007;32(24):2739–44. - PubMed
-
- Ho C, Sucato DJ, Richards BS. Risk factors for the development of delayed infections following posterior spinal fusion and instrumentation in adolescent idiopathic scoliosis patients. Spine (Phila Pa 1976) 2007;32(20):2272–7. - PubMed
-
- Labbe AC, et al. Surgical-site infection following spinal fusion: a case-control study in a children's hospital. Infect Control Hosp Epidemiol. 2003;24(8):591–5. - PubMed
-
- Linam WM, et al. Risk factors associated with surgical site infection after pediatric posterior spinal fusion procedure. Infect Control Hosp Epidemiol. 2009;30(2):109–16. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
