

Bleeding events associated with fibrinolytic therapy and primary percutaneous coronary intervention in patients with STEMI: A systematic review and meta-analysis of randomized controlled trials
- PMID: 27281102
- PMCID: PMC4907680
- DOI: 10.1097/MD.0000000000003877
Bleeding events associated with fibrinolytic therapy and primary percutaneous coronary intervention in patients with STEMI: A systematic review and meta-analysis of randomized controlled trials
Erratum in
-
Erratum: Medicine, Volume 95, Issue 23: Erratum.Medicine (Baltimore). 2016 Jul 18;95(28):e0916. doi: 10.1097/01.md.0000489580.04709.16. eCollection 2016 Jul. Medicine (Baltimore). 2016. PMID: 31265603 Free PMC article.
Abstract
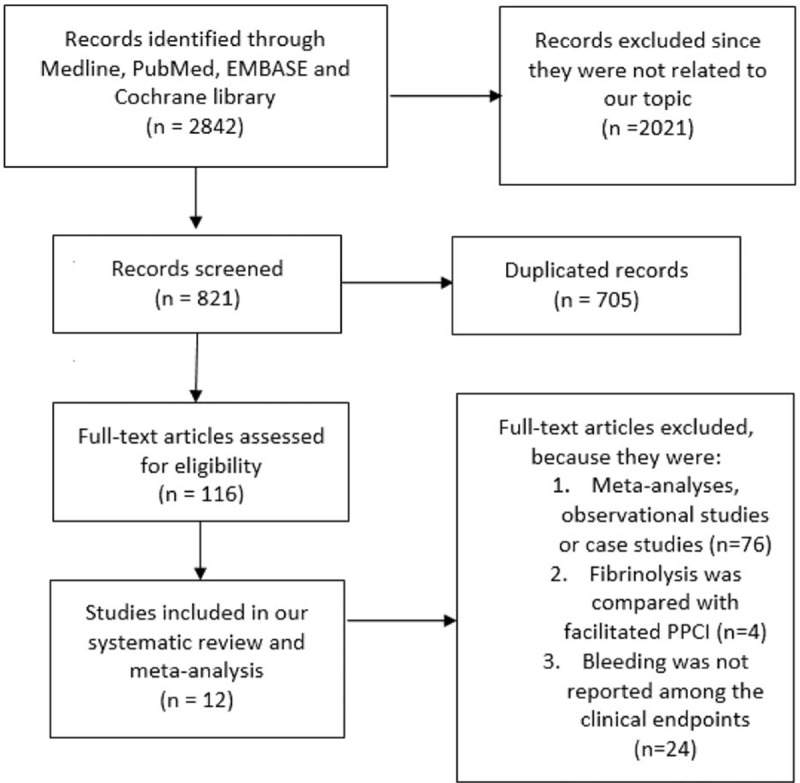
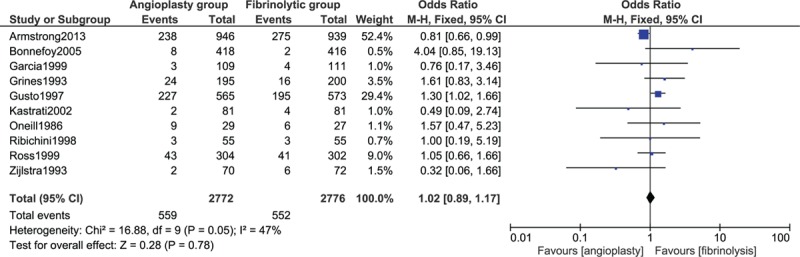
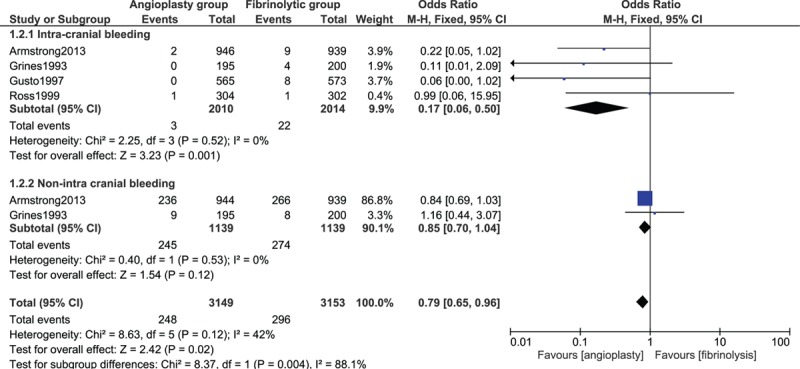
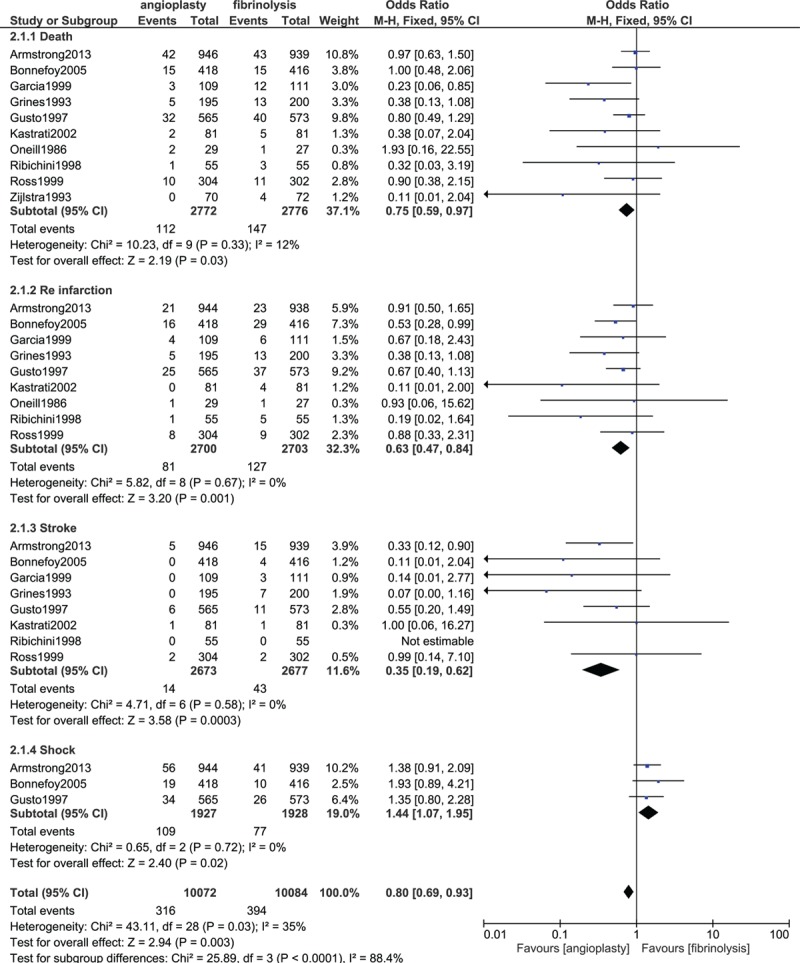
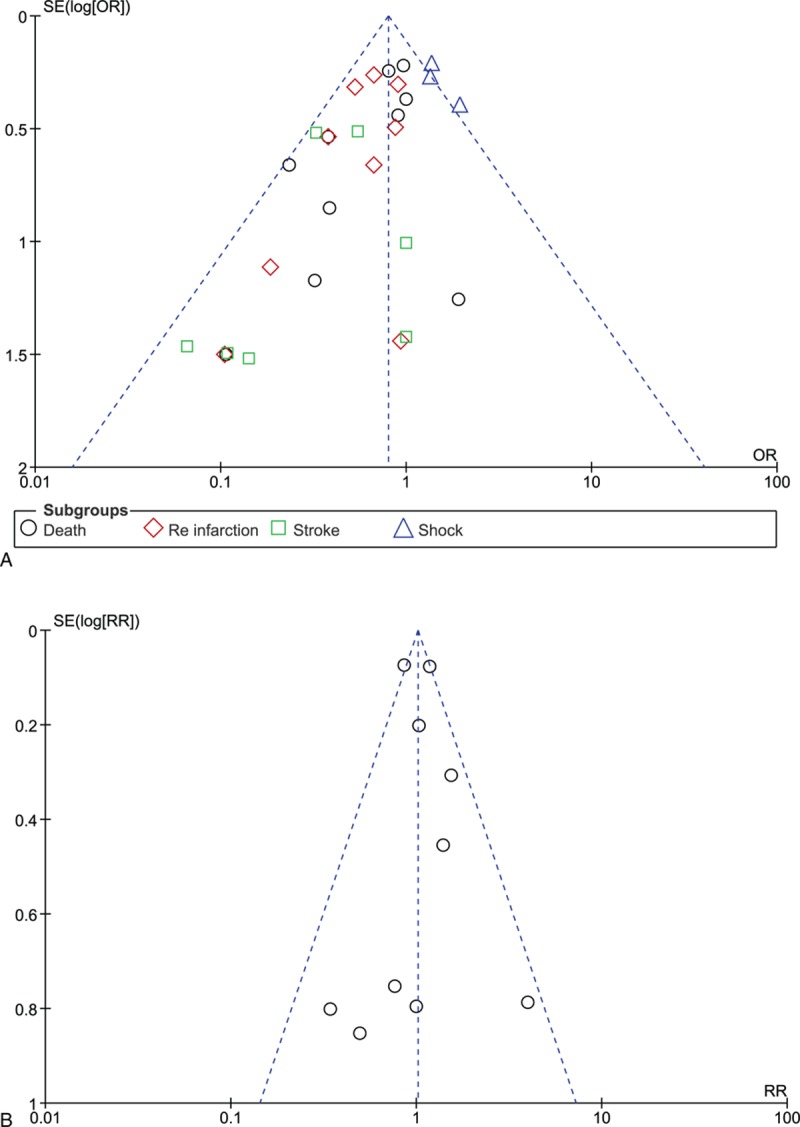
From the year 1986 onwards, several studies have been published focusing on the comparison between fibrinolysis and primary percutaneous coronary intervention (PPCI) in patients with ST segment elevated myocardial infarction (STEMI). However, because antiplatelet and anticoagulating medications are used in approximation, before and during these procedures, bleeding events have been reported to be associated with both reperfusion therapies. This study aimed to compare the bleeding events associated with fibrinolytic therapy and primary angioplasty in patients with STEMI. Randomized controlled trials (RCTs) comparing fibrinolysis and primary angioplasty in patients with STEMI were searched from Medline, PubMed, EMBASE, and the Cochrane databases. Bleeding complications following 30 days from hospitalization were considered as the primary clinical endpoints in this study. Secondary endpoints included all-cause mortality, re-infarction, stroke, and shock. Antiplatelet and anticoagulating drugs used during these 2 different procedures were compared. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated and the pooled analyses were performed with RevMan 5.3 software. Twelve studies involving 10 RCTs consisting of a total number of 5561 patients (2784 patients from the fibrinolysis group and 2777 patients from the PPCI group) were included in this meta-analysis. Our results showed no significant difference in the overall bleeding complications during a 30-day period between these 2 reperfusion therapies with OR 1.02; 95% CI 0.89 to 1.17, P = 0.78. Nonintracranial bleeding was also not statistically significant with OR 0.85; 95% CI 0.70 to 1.04, P = 0.12. However, fibrinolytic therapy was associated with a significantly higher rate of intracranial bleeding with OR 0.17; 95% CI 0.06 to 0.50, P = 0.001 than PPCI. In addition, death, re-infarction, and stroke significantly favored primary angioplasty. According to the results of this study, even if the rate of nonintracranial bleeding was not statistically significant between these 2 reperfusion therapies, fibrinolytic therapy was associated with a significantly higher rate of intracranial bleeding than PPCI. In addition, PPCI was associated with a significantly lower rate of death, reinfarction, and stroke. Therefore, PPCI should be recommended in patients with STEMI, especially in PCI-capable hospitals.
Conflict of interest statement
No writing assistance was required and the authors declare that they have no competing interests.
Figures
References
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. American College of Cardiology Foundation; American Heart Association Task Force on Practice Guidelines; American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines: developed in collaboration with the American College of Emergency Physicians and Society for Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv 2013; 82:E1–E27. - PubMed
-
- Van de Werf F, Barron HV, Armstrong PW, et al. Incidence and predictors of bleeding events after fibrinolytic therapy with fibrin-specific agents: a comparison of TNK-tPA and rt-PA. Eur Heart J 2001; 22:2253–2261. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
