

Malaria: Global progress 2000 - 2015 and future challenges
- PMID: 27282148
- PMCID: PMC4901420
- DOI: 10.1186/s40249-016-0151-8
Malaria: Global progress 2000 - 2015 and future challenges
Abstract
Background: 2015 was the target year for malaria goals set by the World Health Assembly and other international institutions to reduce malaria incidence and mortality. A review of progress indicates that malaria programme financing and coverage have been transformed since the beginning of the millennium, and have contributed to substantial reductions in the burden of disease.
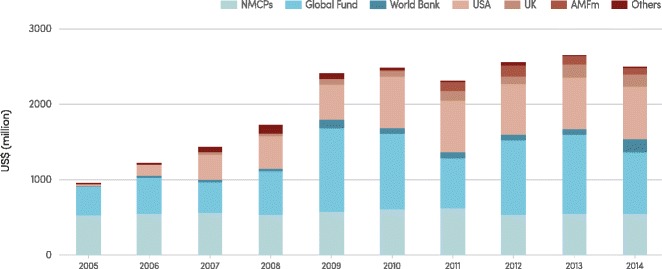
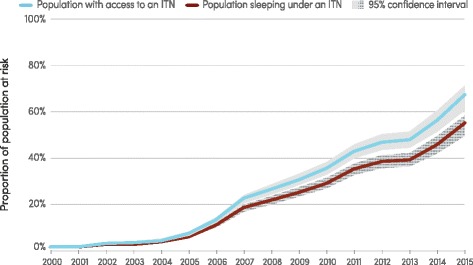
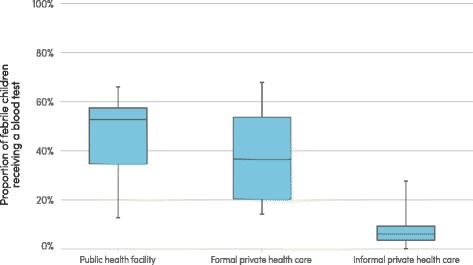
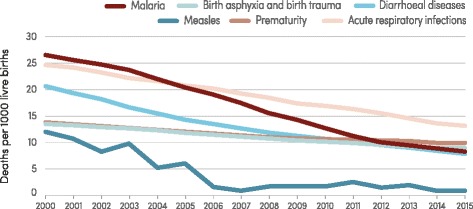
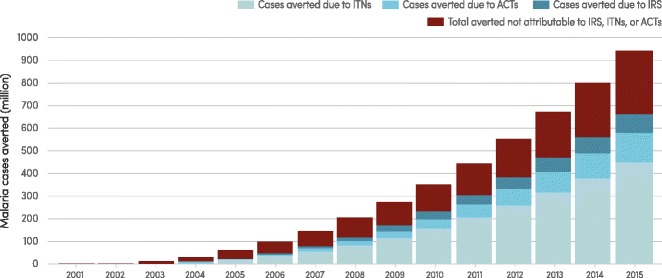
Findings: Investments in malaria programmes increased by more than 2.5 times between 2005 and 2014 from US$ 960 million to US$ 2.5 billion, allowing an expansion in malaria prevention, diagnostic testing and treatment programmes. In 2015 more than half of the population of sub-Saharan Africa slept under insecticide-treated mosquito nets, compared to just 2 % in 2000. Increased availability of rapid diagnostic tests and antimalarial medicines has allowed many more people to access timely and appropriate treatment. Malaria incidence rates have decreased by 37 % globally and mortality rates by 60 % since 2000. It is estimated that 70 % of the reductions in numbers of cases in sub-Saharan Africa can be attributed to malaria interventions.
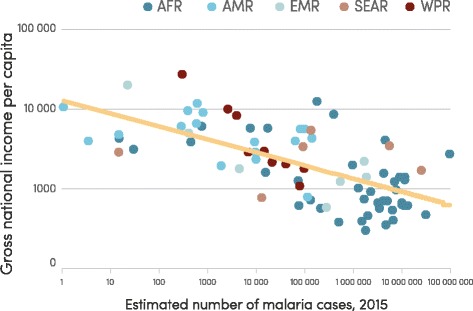
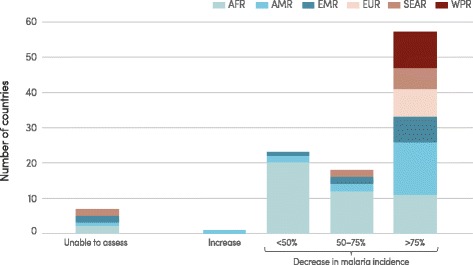
Conclusions: Reductions in malaria incidence and mortality rates have been made in every WHO region and almost every country. However, decreases in malaria case incidence and mortality rates were slowest in countries that had the largest numbers of malaria cases and deaths in 2000; reductions in incidence need to be greatly accelerated in these countries to achieve future malaria targets. Progress is made challenging because malaria is concentrated in countries and areas with the least resourced health systems and the least ability to pay for system improvements. Malaria interventions are nevertheless highly cost-effective and have not only led to significant reductions in the incidence of the disease but are estimated to have saved about US$ 900 million in malaria case management costs to public providers in sub-Saharan Africa between 2000 and 2014. Investments in malaria programmes can not only reduce malaria morbidity and mortality, thereby contributing to the health targets of the Sustainable Development Goals, but they can also transform the well-being and livelihood of some of the poorest communities across the globe.
Keywords: Burden of disease; Elimination; MDG; Malaria; Monitoring and evaluation; Poverty; SDG; Surveillance; Universal health coverage.
Figures
References
-
- World Health Organization. World malaria report 2015. Geneva: World Health Organization; 2015.
-
- World Health Organization. Global technical strategy for malaria 2016–2030. Geneva: World Health Organization; 2015.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
