

Pediatric high-grade glioma: biologically and clinically in need of new thinking
- PMID: 27282398
- PMCID: PMC5464243
- DOI: 10.1093/neuonc/now101
Pediatric high-grade glioma: biologically and clinically in need of new thinking
Abstract
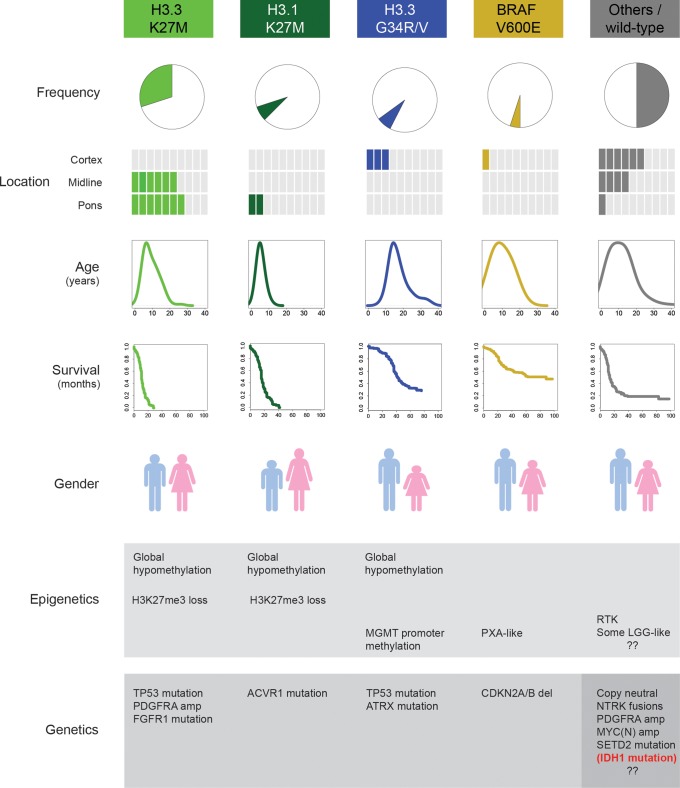
High-grade gliomas in children are different from those that arise in adults. Recent collaborative molecular analyses of these rare cancers have revealed previously unappreciated connections among chromatin regulation, developmental signaling, and tumorigenesis. As we begin to unravel the unique developmental origins and distinct biological drivers of this heterogeneous group of tumors, clinical trials need to keep pace. It is important to avoid therapeutic strategies developed purely using data obtained from studies on adult glioblastoma. This approach has resulted in repetitive trials and ineffective treatments being applied to these children, with limited improvement in clinical outcome. The authors of this perspective, comprising biology and clinical expertise in the disease, recently convened to discuss the most effective ways to translate the emerging molecular insights into patient benefit. This article reviews our current understanding of pediatric high-grade glioma and suggests approaches for innovative clinical management.
Keywords: DIPG; clinical trials; genomics; glioma; pediatric.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology.
Figures
References
-
- Northcott PA, Pfister SM, Jones DT. Next-generation (epi)genetic drivers of childhood brain tumours and the outlook for targeted therapies. Lancet Oncol. 2015;16(6):e293–e302. - PubMed
