

Role of Health Insurance Status in Interfacility Transfers of Patients With ST-Elevation Myocardial Infarction
- PMID: 27282834
- PMCID: PMC4949088
- DOI: 10.1016/j.amjcard.2016.05.007
Role of Health Insurance Status in Interfacility Transfers of Patients With ST-Elevation Myocardial Infarction
Abstract
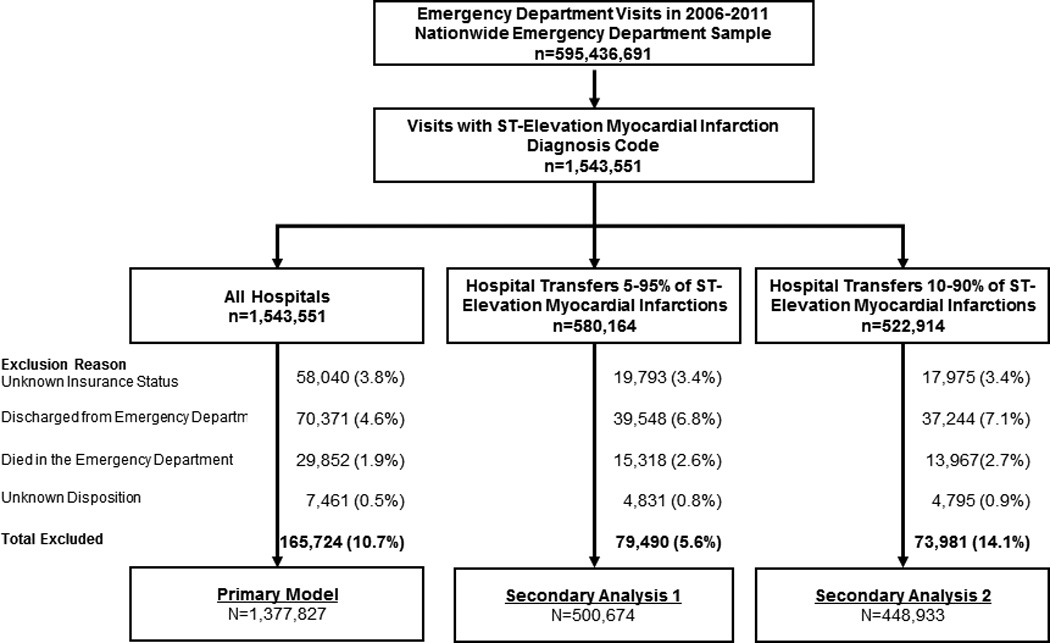
Lack of health insurance is associated with interfacility transfer from emergency departments for several nonemergent conditions, but its association with transfers for ST-elevation myocardial infarction (STEMI), which requires timely definitive care for optimal outcomes, is unknown. Our objective was to determine whether insurance status is a predictor of interfacility transfer for emergency department visits with STEMI. We analyzed data from the 2006 to 2011 Nationwide Emergency Department Sample examining all emergency department visits for patients age 18 years and older with a diagnosis of STEMI and a disposition of interfacility transfer or hospitalization at the same institution. For emergency department visits with STEMI, our multivariate logistic regression model included emergency department disposition status (interfacility transfer vs hospitalization at the same institution) as the primary outcome, and insurance status (none vs any [including Medicare, Medicaid, and private insurance]) as the primary exposure. We found that among 1,377,827 emergency department STEMI visits, including 249,294 (18.1%) transfers, patients without health insurance (adjusted odds ratio 1.6, 95% CI 1.5 to 1.7) were more likely to be transferred than those with insurance. Lack of health insurance status was also an independent risk factor for transfer compared with each subcategory of health insurance, including Medicare, Medicaid, and private insurance. In conclusion, among patients presenting to United States emergency departments with STEMI, lack of insurance was an independent predictor of interfacility transfer. In conclusion, because interfacility transfer is associated with longer delays to definitive STEMI therapy than treatment at the same facility, lack of health insurance may lead to important health disparities among patients with STEMI.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- James ML, Grau-Sepulveda MV, Olson DM, Smith EE, Hernandez AF, Peterson ED, Schwamm LH, Bhatt DL, Fonarow GC. Insurance status and outcome after intracerebral hemorrhage: findings from Get With The Guidelines-stroke. J Stroke Cerebrovasc Dis. 2014;23:283–292. - PubMed
-
- Wang TY, Nallamothu BK, Krumholz HM, Li S, Roe MT, Jollis JG, Jacobs AK, Holmes DR, Peterson ED, Ting HH. Association of door-in to door-out time with reperfusion delays and outcomes among patients transferred for primary percutaneous coronary intervention. JAMA. 2011;305:2540–2547. - PubMed
-
- Antman EM. Time is muscle: translation into practice. Journal of the American College of Cardiology. 2008;52:1216–1221. - PubMed
-
- HCUP Nationwide Emergency Department Sample (NEDS) Healthcare Cost and Utilization Project (HCUP) Agency for Healthcare Research and Quality; Rockville, MD: 2006 – 2011. www.hcup-us.ahrq.gov/nedsoverview.jsp. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
