

A New Method to Increase Ultrafiltration in Peritoneal Dialysis: Steady Concentration Peritoneal Dialysis
- PMID: 27282854
- PMCID: PMC5033632
- DOI: 10.3747/pdi.2016.00007
A New Method to Increase Ultrafiltration in Peritoneal Dialysis: Steady Concentration Peritoneal Dialysis
Abstract
♦
Background: Peritoneal dialysis (PD) has limited power for liquid extraction (ultrafiltration), so fluid overload remains a major cause of treatment failure. ♦
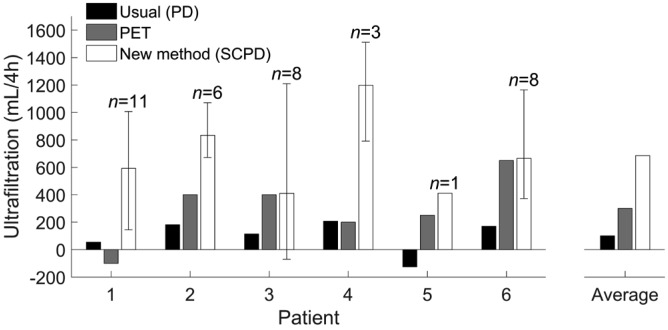
Methods: We present steady concentration peritonal dialysis (SCPD), which increases ultrafiltration of PD exchanges by maintaining a constant peritoneal glucose concentration. This is achieved by infusing 50% glucose solution at a constant rate (typically 40 mL/h) during the 4-hour dwell of a 2-L 1.36% glucose exchange. We treated 21 fluid overload episodes on 6 PD patients with high or average-high peritoneal transport characteristics who refused hemodialysis as an alternative. Each treatment consisted of a single session with 1 to 4 SCPD exchanges (as needed). ♦
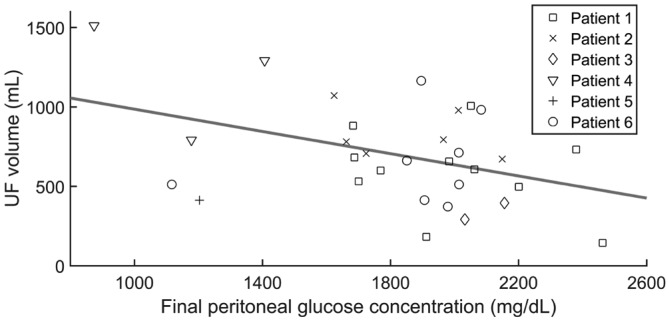
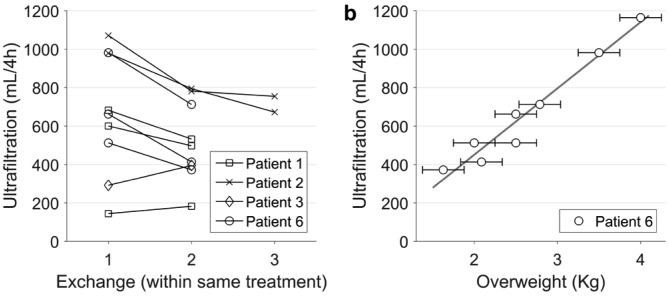
Results: Ultrafiltration averaged 653 ± 363 mL/4 h - twice the ultrafiltration of the peritoneal equilibration test (PET) (300 ± 251 mL/4 h, p < 0.001) and 6-fold the daily ultrafiltration (100 ± 123 mL/4 h, p < 0.001). Serum and peritoneal glucose stability and dialysis efficacy were excellent (glycemia 126 ± 25 mg/dL, peritoneal glucose 1,830 ± 365 mg/dL, D/P creatinine 0.77 ± 0.08). The treatment reversed all episodes of fluid overload, avoiding transfer to hemodialysis. Ultrafiltration was proportional to fluid overload (p < 0.01) and inversely proportional to final peritoneal glucose concentration (p < 0.05). ♦
Conclusion: This preliminary clinical experience confirms the potential of SCPD to safely and effectively increase ultrafiltration of PD exchanges. It also shows peritoneal transport in a new dynamic context, enhancing the influence of factors unrelated to the osmotic gradient.
Keywords: Ultrafiltration; fluid overload; fluid transport kinetics; glucose concentration; hydrostatic pressure; intraperitoneal pressure; osmotic gradient; technique failure.
Copyright © 2016 International Society for Peritoneal Dialysis.
Figures
Similar articles
-
Volume-Based Peritoneal Dialysis Prescription Guide to Achieve Adequacy Targets.Perit Dial Int. 2016 Mar-Apr;36(2):188-95. doi: 10.3747/pdi.2014.00255. Epub 2015 Aug 20. Perit Dial Int. 2016. PMID: 26293841 Free PMC article.
-
Should peritoneal resting be advised in ultrafiltration failure associated with a fast peritoneal solute transport status?Perit Dial Int. 2014 Nov-Dec;34(7):695-7. doi: 10.3747/pdi.2014.00196. Perit Dial Int. 2014. PMID: 25520482 Free PMC article. Review. No abstract available.
-
Computer simulations of steady concentration peritoneal dialysis.Perit Dial Int. 2020 Jan;40(1):76-83. doi: 10.1177/0896860819878635. Perit Dial Int. 2020. PMID: 32063154
-
A Large Intraperitoneal Residual Volume Hampers Adequate Volumetric Assessment of Osmotic Conductance to Glucose.Perit Dial Int. 2018 Sep-Oct;38(5):356-362. doi: 10.3747/pdi.2017.00219. Epub 2018 Apr 19. Perit Dial Int. 2018. PMID: 29674410
-
Icodextrin Versus Glucose Solutions for the Once-Daily Long Dwell in Peritoneal Dialysis: An Enriched Systematic Review and Meta-analysis of Randomized Controlled Trials.Am J Kidney Dis. 2020 Jun;75(6):830-846. doi: 10.1053/j.ajkd.2019.10.004. Epub 2020 Feb 4. Am J Kidney Dis. 2020. PMID: 32033860
Cited by
-
A Uremic Pig Model for Peritoneal Dialysis.Toxins (Basel). 2022 Sep 14;14(9):635. doi: 10.3390/toxins14090635. Toxins (Basel). 2022. PMID: 36136573 Free PMC article.
-
Risk, Severity, and Predictors of Obstructive Sleep Apnea in Hemodialysis and Peritoneal Dialysis Patients.Int J Environ Res Public Health. 2018 Oct 26;15(11):2377. doi: 10.3390/ijerph15112377. Int J Environ Res Public Health. 2018. PMID: 30373203 Free PMC article.
References
-
- Liberek T, Renke M, Skonieczny B, Kotewicz K, Kowalewska J, Chmielewski M, et al. Therapy outcome in peritoneal dialysis patients transferred from haemodialysis. Nephrol Dial Transplant 2009; 24:2889–94. - PubMed
-
- Tietelbaum I. Ultrafiltration failure in peritoneal dialysis. A pathophysiologic approach. Blood Purif 2015; 39:70–3. - PubMed
-
- Pyle WK. Mass Transfer in Peritoneal Dialysis. Ph D Disertation Univ of Texas; 1981.
- Cited by Popovich RP, Moncrief JW. 5 Transport kinetics. In: Nolph KD, ed. Peritoneal Dialysis. Second edition Dordrecht: Martinus Nijhoff Publishers; 1985:122–58.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
