

Aortic Dissection in Patients With Genetically Mediated Aneurysms: Incidence and Predictors in the GenTAC Registry
- PMID: 27282895
- PMCID: PMC5040186
- DOI: 10.1016/j.jacc.2016.03.570
Aortic Dissection in Patients With Genetically Mediated Aneurysms: Incidence and Predictors in the GenTAC Registry
Abstract
Background: Aortic dissection (AoD) is a serious complication of thoracic aortic aneurysm (TAA). Relative risk for AoD in relation to TAA etiology, incidence, and pattern after prophylactic TAA surgery are poorly understood.
Objectives: This study sought to determine the incidence, pattern, and relative risk for AoD among patients with genetically associated TAA.
Methods: The population included adult GenTAC participants without AoD at baseline. Standardized core laboratory tests classified TAA etiology and measured aortic size. Follow-up was performed for AoD.
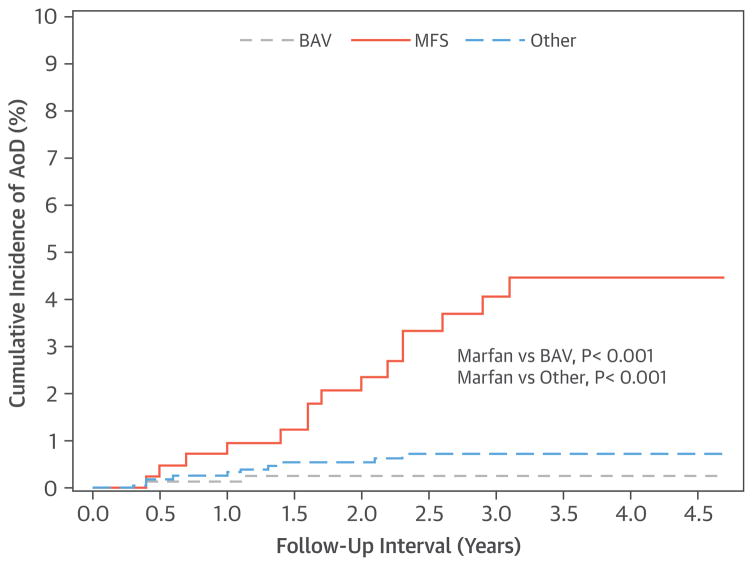
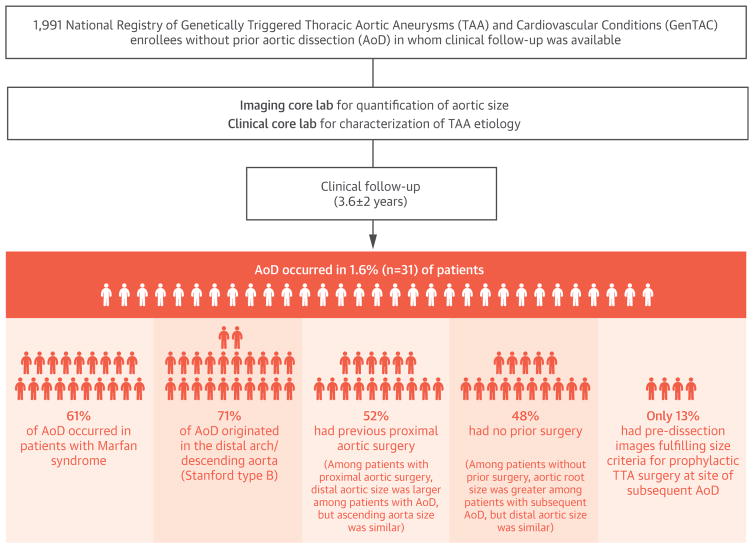
Results: Bicuspid aortic valve (BAV) (39%) and Marfan syndrome (MFS) (22%) were the leading diagnoses in the studied GenTAC participants (n = 1,991). AoD occurred in 1.6% over 3.6 ± 2.0 years; 61% of AoD occurred in patients with MFS. Cumulative AoD incidence was 6-fold higher among patients with MFS (4.5%) versus others (0.7%; p < 0.001). MFS event rates were similarly elevated versus those in patients with BAV (0.3%; p < 0.001). AoD originated in the distal arch or descending aorta in 71%; 52% of affected patients, including 68% with MFS, had previously undergone aortic grafting. In patients with proximal aortic surgery, distal aortic size (descending thoracic, abdominal aorta) was larger among patients with AoD versus those without AoD (both p < 0.05), whereas the ascending aorta size was similar. Conversely, in patients without previous surgery, aortic root size was greater in patients with subsequent AoD (p < 0.05), whereas distal aortic segments were of similar size. MFS (odds ratio: 7.42; 95% confidence interval: 3.43 to 16.82; p < 0.001) and maximal aortic size (1.86 per cm; 95% confidence interval: 1.26 to 2.67; p = 0.001) were independently associated with AoD. Only 4 of 31 (13%) patients with AoD had pre-dissection images that fulfilled size criteria for prophylactic TAA surgery at a subsequent AoD site.
Conclusions: Among patients with genetically associated TAA, MFS augments risk for AoD even after TAA grafting. Although increased aortic size is a risk factor for subsequent AoD, events typically occur below established thresholds for prophylactic TAA repair.
Keywords: Marfan syndrome; aortic aneurysm; aortic dissection; bicuspid aortic valve.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
The Natural History of Thoracic Aortic Disease: So Much Left to Learn.J Am Coll Cardiol. 2016 Jun 14;67(23):2755-2757. doi: 10.1016/j.jacc.2016.04.007. J Am Coll Cardiol. 2016. PMID: 27282896 No abstract available.
-
Genetically Triggered Thoracic Aortic Aneurysms and Cardiovascular Conditions (GenTAC) registry predicting predictors for aortic dissection: a new thought around the corner?J Thorac Dis. 2016 Sep;8(9):E1093-E1095. doi: 10.21037/jtd.2016.08.71. J Thorac Dis. 2016. PMID: 27747073 Free PMC article. No abstract available.
References
-
- Hagan PG, Nienaber CA, Isselbacher EM, et al. The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA. 2000;283:897–903. - PubMed
-
- Mehta RH, Suzuki T, Hagan PG, et al. Predicting death in patients with acute type A aortic dissection. Circulation. 2002;105:200–6. - PubMed
-
- Roman MJ, Rosen SE, Kramer-Fox R, Devereux RB. Prognostic significance of the pattern of aortic root dilation in the Marfan syndrome. J Am Coll Cardiol. 1993;22:1470–6. - PubMed
-
- Michelena HI, Khanna AD, Mahoney D, et al. Incidence of aortic complications in patients with bicuspid aortic valves. JAMA. 2011;306:1104–12. - PubMed
-
- Detaint D, Michelena HI, Nkomo VT, et al. Aortic dilatation patterns and rates in adults with bicuspid aortic valves: a comparative study with Marfan syndrome and degenerative aortopathy. Heart. 2014;100:126–34. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
