

Plasma interleukin-6 concentrations, metabolic dysfunction, and asthma severity: a cross-sectional analysis of two cohorts
- PMID: 27283230
- PMCID: PMC5007068
- DOI: 10.1016/S2213-2600(16)30048-0
Plasma interleukin-6 concentrations, metabolic dysfunction, and asthma severity: a cross-sectional analysis of two cohorts
Erratum in
-
Corrections.Lancet Respir Med. 2018 Mar;6(3):e10. doi: 10.1016/S2213-2600(18)30073-0. Lancet Respir Med. 2018. PMID: 29508707 No abstract available.
Abstract
Background: Severe asthma is a complex heterogeneous disease associated with older age and obesity. The presence of eosinophilic (type 2) inflammation in some but not all patients with severe asthma predicts responsiveness to current treatments, but new treatment approaches will require a better understanding of non-type 2 mechanisms of severe asthma. We considered the possibility that systemic inflammation, which arises in subgroups of obese and older patients, increases the severity of asthma. Interleukin-6 (IL-6) is a biomarker of systemic inflammation and metabolic dysfunction, and we aimed to explore the association between IL-6 concentrations, metabolic dysfunction, and asthma severity.
Methods: In this cross-sectional analysis, patients were recruited from two cohorts: mainly non-severe asthmatics from the University of California San Francisco (UCSF) and mainly severe asthmatics from the Severe Asthma Research Program (SARP). We generated a reference range for plasma IL-6 in a cohort of healthy control patients. We compared the clinical characteristics of asthmatics with plasma IL-6 concentrations above (IL-6 high) and below (IL-6 low) the upper 95% centile value for plasma IL-6 concentration in the healthy cohort. We also compared how pulmonary function, frequency of asthma exacerbations, and frequency of severe asthma differed between IL-6 low and IL-6 high asthma populations in the two asthma cohorts.
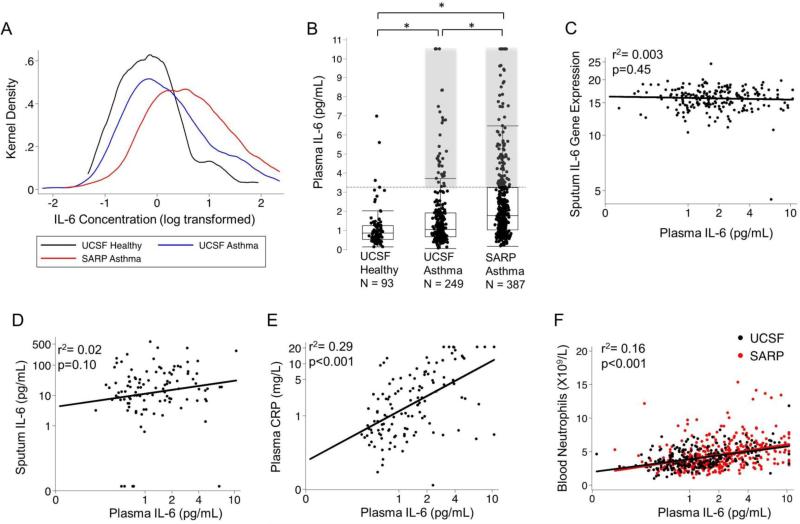
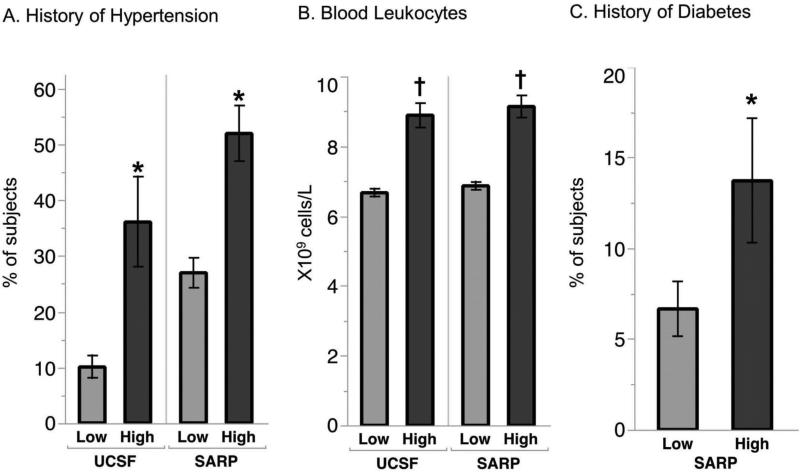
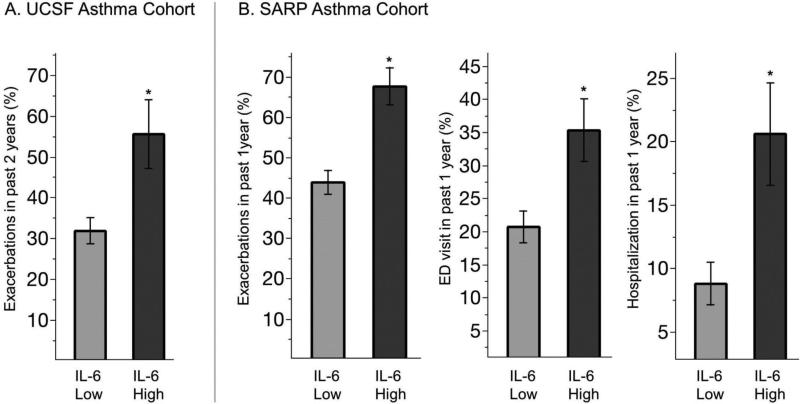
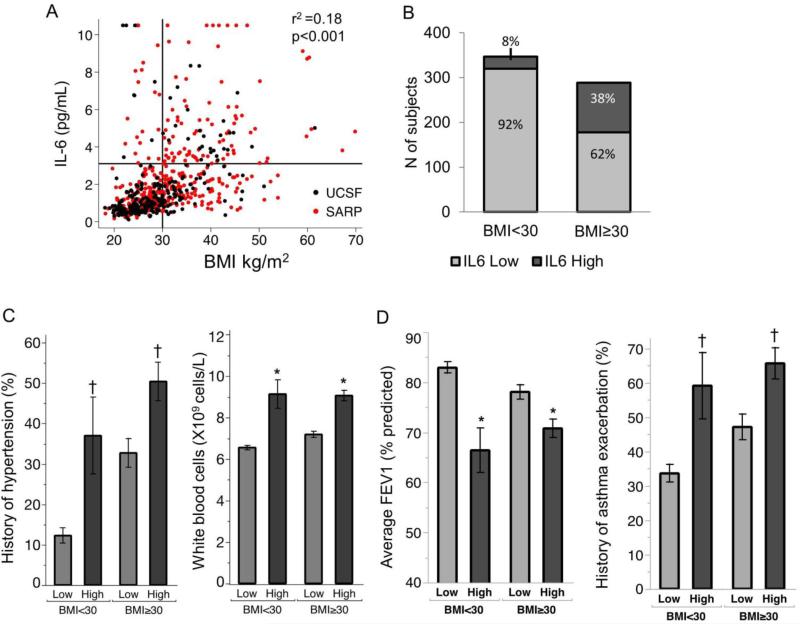
Findings: Between Jan 1, 2005, and Dec 31, 2014, we recruited 249 patients from UCSF and between Nov 1, 2012, and Oct 1, 2014, we recruited 387 patients from SARP. The upper 95th centile value for plasma IL-6 concentration in the healthy cohort (n=93) was 3·1 pg/mL, and 14% (36/249) of UCSF cohort and 26% (102/387) of the SARP cohort had plasma IL-6 concentrations above this upper limit. The IL-6 high patients in both asthma cohorts had a significantly higher average BMI (p<0·0001) and a higher prevalence of hypertension (p<0·0001) and diabetes (p=0·04) than the IL-6 low patients. IL-6 high patients also had significantly worse lung function and more frequent asthma exacerbations than IL-6 low patients (all p values <0·0001). Although 80% (111/138) of IL-6 high asthmatic patients were obese, 62% (178/289) of obese asthmatic patients were IL-6 low. Among obese patients, the forced expiratory volume in 1 s (FEV1) was significantly lower in IL-6 high than in IL-6 low patients (mean percent predicted FEV1=70·8% [SD 19·5] vs 78·3% [19·7]; p=0·002), and the percentage of patients reporting an asthma exacerbation in the past 1-2 years was higher in IL-6 high than in IL-6 low patients (66% [73/111] vs 48% [85/178]; p=0·003). Among non-obese asthmatics, FEV1 values and the frequency of asthma exacerbations within the past 1-2 years were also significantly worse in IL-6 high than in IL-6 low patients (mean FEV1 66·4% [SD 23·1] vs 83·2% [20·4] predicted; p<0·0001; 59% [16/27] vs 34% [108/320]; p=0·01).
Interpretation: Systemic IL-6 inflammation and clinical features of metabolic dysfunction, which occur most commonly in a subset of obese asthma patients but also in a small subset of non-obese patients, are associated with more severe asthma. These data provide strong rationale to undertake clinical trials of IL-6 inhibitors or treatments that reduce metabolic dysfunction in a subset of patients with severe asthma. Plasma IL-6 is a biomarker that could guide patient stratification in these trials.
Funding: NIH and the Parker B Francis Foundation.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Metabolic dysfunction: mediator of the link between obesity and asthma?Lancet Respir Med. 2016 Jul;4(7):533-534. doi: 10.1016/S2213-2600(16)30104-7. Epub 2016 Jun 6. Lancet Respir Med. 2016. PMID: 27283229 No abstract available.
References
-
- Yokoyama A, Kohno N, Fujino S, Hamada H, Inoue Y, Fujioka S, et al. Circulating interleukin-6 levels in patients with bronchial asthma. Am J Respir Crit Care Med. 1995 May;151(5):1354–1358. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U10 HL109257/HL/NHLBI NIH HHS/United States
- UL1 TR000427/TR/NCATS NIH HHS/United States
- K12 HL119997/HL/NHLBI NIH HHS/United States
- U10 HL109250/HL/NHLBI NIH HHS/United States
- U10 HL109164/HL/NHLBI NIH HHS/United States
- U10 HL109086/HL/NHLBI NIH HHS/United States
- U10 HL109168/HL/NHLBI NIH HHS/United States
- R01 HL080414/HL/NHLBI NIH HHS/United States
- U10 HL109172/HL/NHLBI NIH HHS/United States
- U10 HL064313/HL/NHLBI NIH HHS/United States
- R01 HL122531/HL/NHLBI NIH HHS/United States
- U19 AI077439/AI/NIAID NIH HHS/United States
- U10 HL109152/HL/NHLBI NIH HHS/United States
- U10 HL109146/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
