

The sphenoid sinus, foramen rotundum and vidian canal: a radiological study of anatomical relationships
- PMID: 27283380
- PMCID: PMC9442688
- DOI: 10.1016/j.bjorl.2016.04.013
The sphenoid sinus, foramen rotundum and vidian canal: a radiological study of anatomical relationships
Abstract
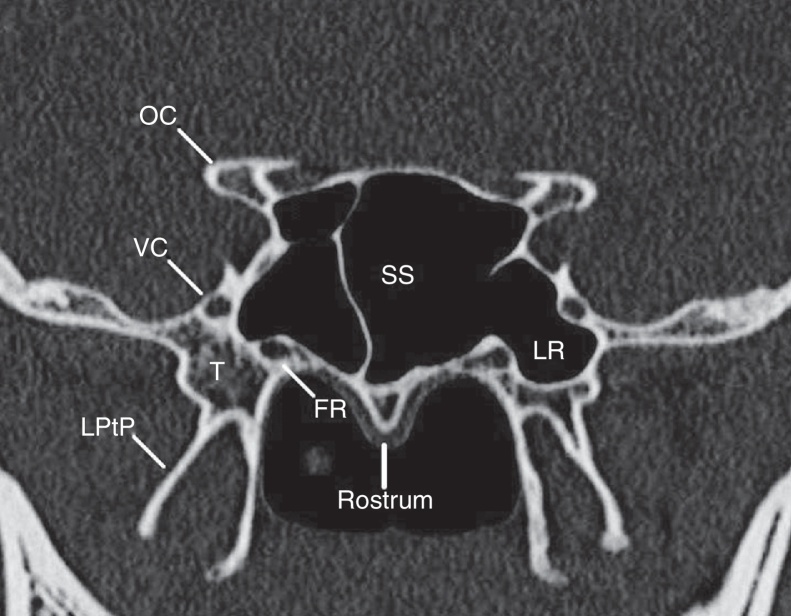
Introduction: The sphenoid sinus is an important structure in ventral skull base surgeries that is surrounded by several vital anatomical structures including the internal carotid arteries, optic nerve and cranial nerves inside the cavernous sinus. In addition, the foramen rotundum is a small canal deeply situated in the base of the skull, which represents the way for exit of the maxillary nerve. Understanding of the sphenoid bone anatomical relationships is central to the expanded endonasal approaches to the skull base.
Objective: To record and analyze the measurement indexes of the sphenoid sinus and foramen rotundum in the coronal plane of normal computer tomography scans.
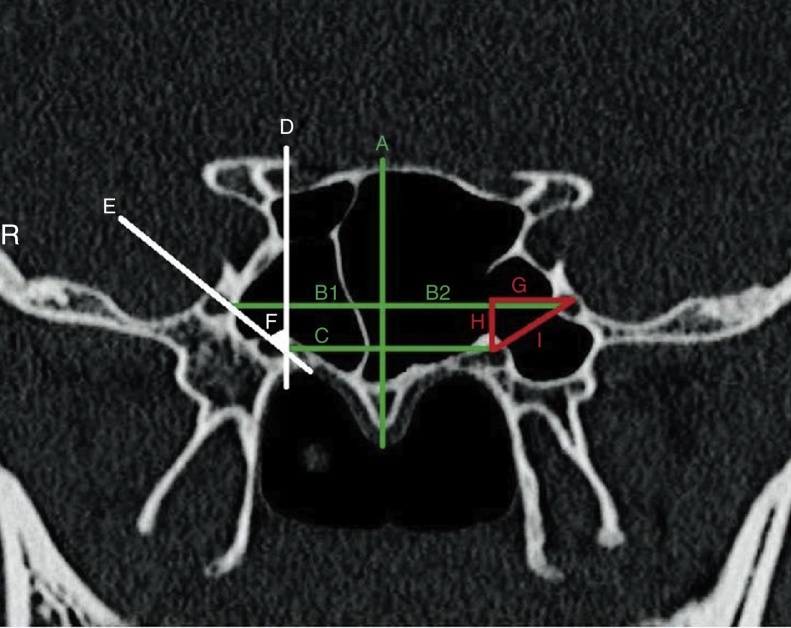
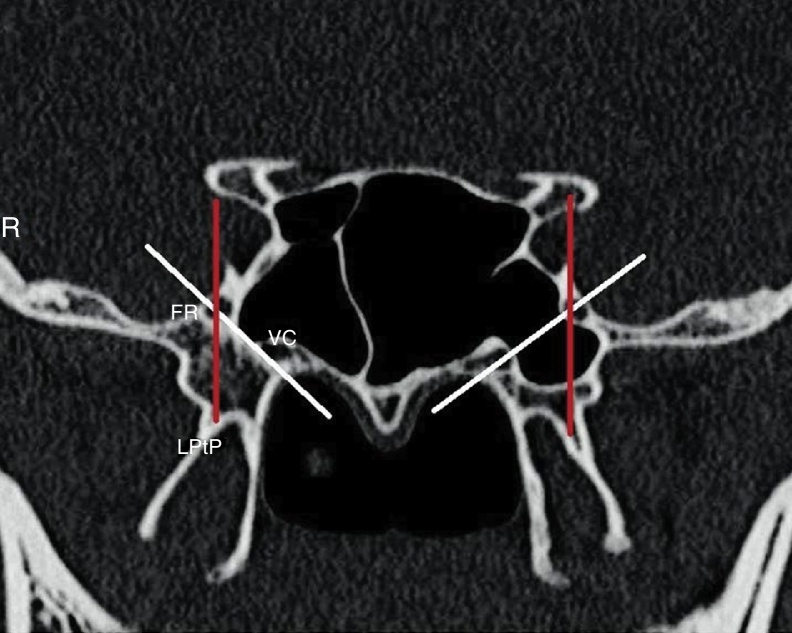
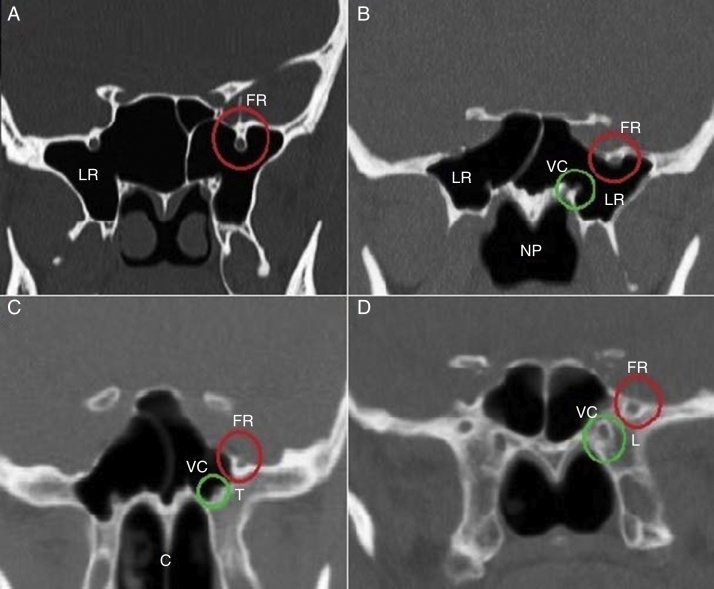
Methods: Patients underwent paranasal sinuses computer tomography scan from June 2014 to November 2015 were retrospectively entered this cross-sectional study. We obtained several morphometric measurements from both the right and left sides using computer software. We also classified foramen rotundum and vidian canal types and determined position of the foramen rotundum regarding to base of lateral pterygoid plate.
Results: One-hundred patients with the mean age of 38.56±18.51 years entered this study. Mean bilateral FR distances were 38.48±3.87mm. Average right and left FRs distances to midline were 19.00±2.07 and 19.34±2.17mm, respectively (p=0.03). Twenty-eight cases (28%) had type I vidian canal, 48% and 24% had type II and III vidian canals, respectively. Four patients (4%) had type I rotundum foramen, 28% and 44% had type IIa and IIb, respectively and 24% had type III rotundum foramen. The position of foramen rotundums regarding to the base of lateral pterygoid plate was online in 50% of cases, medially placed in 47% and laterally placed in 3% of cases.
Conclusion: The results of this study can be used to provide a better anatomical understanding of the area, which is necessary for endoscopic skull base surgeons.
Introdução: O seio esfenoidal (SE) é uma estrutura importante em cirurgias da base do crânio, que está cercada por várias estruturas anatômicas vitais, como as artérias carótidas internas, o nervo óptico e os nervos cranianos no interior do seio cavernoso. Além disso, o forame redondo (FR) é um pequeno canal profundamente situado na base do crânio, que representa a forma de saída do nervo maxilar. Compreender as relações anatômicas do osso esfenoidal é fundamental para as abordagens endonasais expandidas da base do crânio.
Objetivo: Registrar e analisar os índices de medição do SE e FR no plano coronal de exames normais de TC.
Método: Os pacientes que foram submetidos a TC dos seios paranasais (SPN) de junho de 2014 a novembro 2015 foram retrospectivamente incluídos neste estudo transversal. Obtivemos várias medidas morfométricas de ambos os lados direito e esquerdo usando software de computador. Também classificamos os tipos de FR e canal pterigoideo (CP) e determinamos a posição do FR em relação à base da placa pterigoide lateral.
Resultados: Cem pacientes com a média de idade de 38,56 ± 18,51 anos foram incluídos neste estudo. As distâncias médias bilaterais de FR foram de 38,48 ± 3,87 milímetros. As distâncias médias direita e esquerda dos FR até a linha média foram de 19,00 ± 2,07 e 19,34 ± 2,17 mm, respectivamente (p = 0,03). Vinte e oito casos (28%) tinham canal pterigoideo do tipo I, 48% e 24% canais pterigoideos de tipo II e III, respectivamente. Quatro pacientes (4%) tinham forame redondo do tipo I, 28% e 44% do tipo II-a e II-b, respectivamente, e 24% forame redondo do tipo III. A posição dos FR em relação à base da placa pterigoide lateral era em linha em 50% dos casos, medialmente posicionados em 47% e lateralmente posicionados em 3% dos casos.
Conclusão: Os resultados deste estudo podem ser utilizados para promover uma melhor compreensão anatômica da área, necessária para cirurgias endoscópicas da base do crânio.
Keywords: Canal pterigoideo; Forame redondo; Foramen rutundum; Seio esfenoidal; Sphenoid sinus; Vidian canal.
Copyright © 2016. Published by Elsevier Editora Ltda.
Figures
References
-
- Vaezi A., Cardenas E., Pinheiro-Neto C., Paluzzi A., Branstetter B.Ft., Gardner P.A., et al. Classification of sphenoid sinus pneumatization: relevance for endoscopic skull base surgery. Laryngoscope. 2015;125:577–581. - PubMed
-
- Citardi M.J., Gallivan R.P., Batra P.S., Maurer C.R., Jr., Rohlfing T., Roh H.J., et al. Quantitative computer-aided computed tomography analysis of sphenoid sinus anatomical relationships. Am J Rhinol. 2004;18:173–178. - PubMed
-
- Wang J., Bidari S., Inoue K., Yang H., Rhoton A., Jr. Extensions of the sphenoid sinus: a new classification. Neurosurgery. 2010;66:797–816. - PubMed
-
- Vescan A.D., Snyderman C.H., Carrau R.L., Mintz A., Gardner P., Branstetter Bt., et al. Vidian canal: analysis and relationship to the internal carotid artery. Laryngoscope. 2007;117:1338–1342. - PubMed
-
- Budu V., Mogoanta C.A., Fanuta B., Bulescu I. The anatomical relations of the sphenoid sinus and their implications in sphenoid endoscopic surgery. Rom J Morphol Embryol. 2013;54:13–16. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
