

Why, when and how should immunosuppressive therapy considered in patients with immunoglobulin A nephropathy?
- PMID: 27283488
- PMCID: PMC5054563
- DOI: 10.1111/cei.12823
Why, when and how should immunosuppressive therapy considered in patients with immunoglobulin A nephropathy?
Abstract
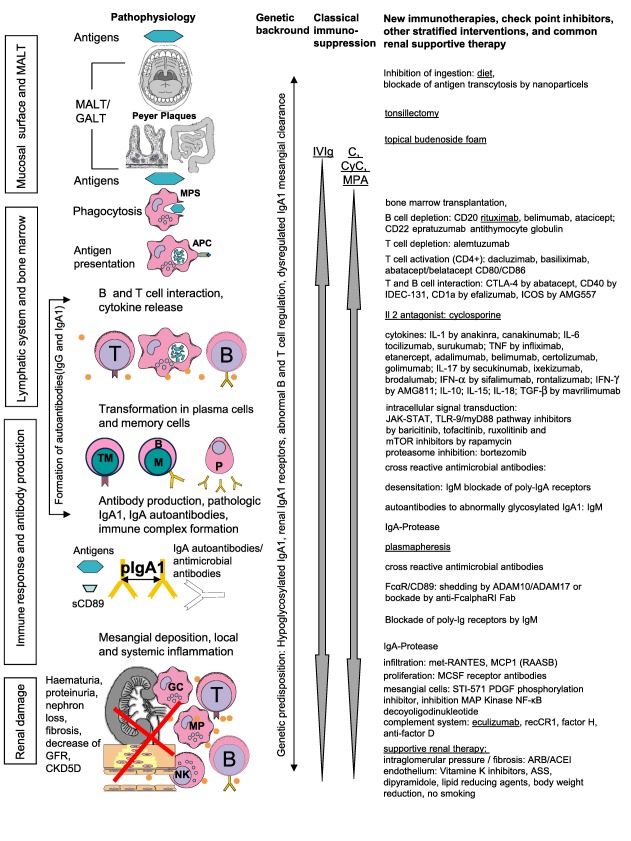
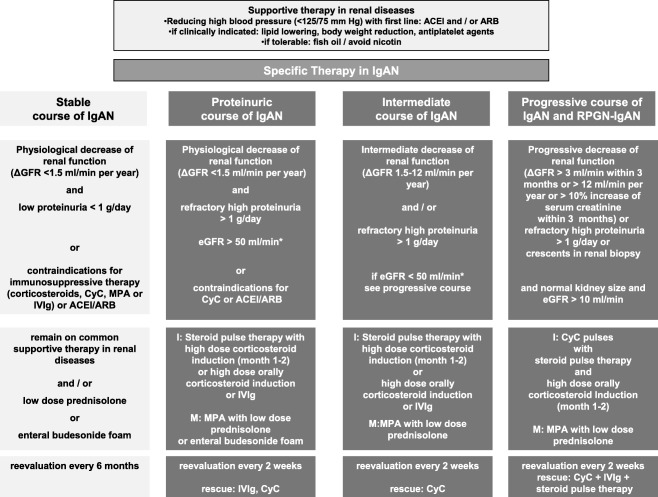
IgA nephropathy (IgAN) is the most common primary glomerulonephritis worldwide. Lifelong mesangial deposition of IgA1 complexes subsist inflammation and nephron loss, but the complex pathogenesis in detail remains unclear. In regard to the heterogeneous course, classical immunosuppressive and specific therapeutic regimens adapted to the loss of renal function will here be discussed in addition to the essential common renal supportive therapy. Renal supportive therapy alleviates secondary, surrogate effects or sequelae on renal function and proteinuria of high intraglomerular pressure and subsequent nephrosclerosis by inhibition of the renin angiotensin system (RAASB). In patients with physiological (ΔGFR < 1·5 ml/min/year) or mild (ΔGFR 1·5-5 ml/min/year) decrease of renal function and proteinuric forms (> 1 g/day after RAASB), corticosteroids have shown a reduction of proteinuria and might protect further loss of renal function. In patients with progressive loss of renal function (ΔGFR > 3 ml/min within 3 months) or a rapidly progressive course with or without crescents in renal biopsy, cyclophosphamide with high-dose corticosteroids as induction therapy and azathioprine maintenance has proved effective in one randomized controlled study of a homogeneous cohort in loss of renal function (ΔGFR). Mycophenolic acid provided further maintenance in non-randomized trials. Differentiated, precise, larger, randomized, placebo-controlled studies focused on the loss of renal function in the heterogeneous forms of IgAN are still lacking. Prospectively, fewer toxic agents will be necessary in the treatment of IgAN.
Keywords: IgA nephropathy; corticosteroids; cyclophosphamide; high dose intravenous immunoglobulines; mycophenolic acid.
© 2016 British Society for Immunology.
Figures
References
-
- Berger J, Hinglais N. Les dépôts intercapillaires d'IgA‐IgG [Intercapillary deposits of IgA]. J Urol Nephrol (Paris) 1968; 74:694–5. - PubMed
-
- Czock D, Keller F, Rasche FM et al Pharmacokinetics and pharmacodynamics of systemically administered glucocorticoids. Clin Pharmacokinet 2005; 44:61–98. - PubMed
-
- Rostoker G, Desvaux‐Belghiti D, Pilatte Y et al High‐dose immunoglobulin therapy for severe IgA nephropathy and Henoch–Schonlein purpura. Ann Intern Med 1994; 120:476–84. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
