

Management of Intracranial Meningiomas Using Keyhole Techniques
- PMID: 27284496
- PMCID: PMC4889455
- DOI: 10.7759/cureus.588
Management of Intracranial Meningiomas Using Keyhole Techniques
Abstract
Background: Keyhole craniotomies are increasingly being used for lesions of the skull base. Here we review our recent experience with these approaches for resection of intracranial meningiomas.
Methods: Clinical and operative data were gathered on all patients treated with keyhole approaches by the senior author from January 2012 to June 2013. Thirty-one meningiomas were resected in 27 patients, including 9 supratentorial, 5 anterior fossa, 7 middle fossa, 6 posterior fossa, and 4 complex skull base tumors. Twenty-nine tumors were WHO Grade I, and 2 were Grade II.
Results: The mean operative time was 8 hours, 22 minutes (range, 2:55-16:14) for skull-base tumors, and 4 hours, 27 minutes (range, 1:45-7:13) for supratentorial tumors. Simpson Resection grades were as follows: Grade I = 8, II = 8, III = 1, IV = 15, V = 0. The median postoperative hospital stay was 4 days (range, 1-20 days). In the 9 patients presenting with some degree of visual loss, 7 saw improvement or complete resolution. In the 6 patients presenting with cranial nerve palsies, 4 experienced improvement or resolution of the deficit postoperatively. Four patients experienced new neurologic deficits, all of which were improved or resolved at the time of the last follow-up. Technical aspects and surgical nuances of these approaches for management of intracranial meningiomas are discussed.
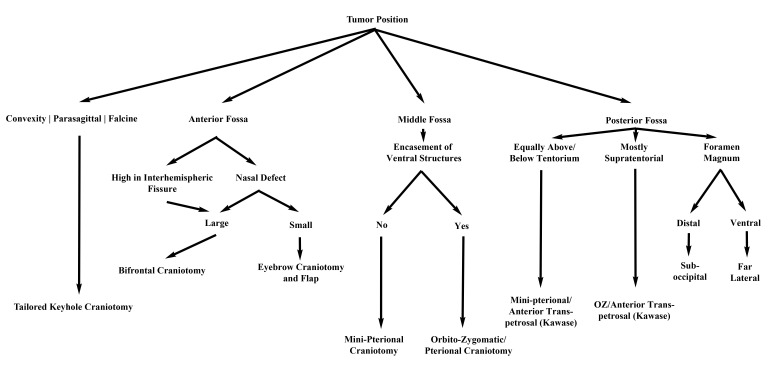
Conclusions: With careful preoperative evaluation, keyhole approaches can be utilized singly or in combination to manage meningiomas in a wide variety of locations with satisfactory results.
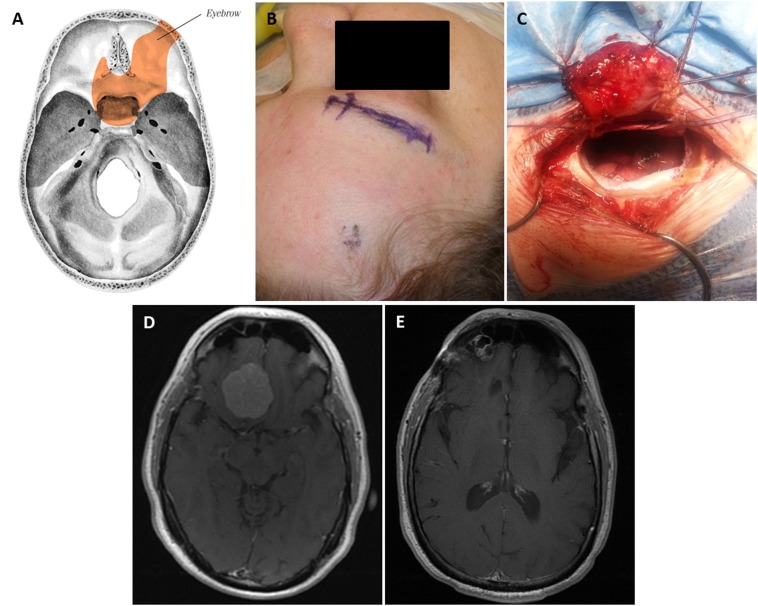
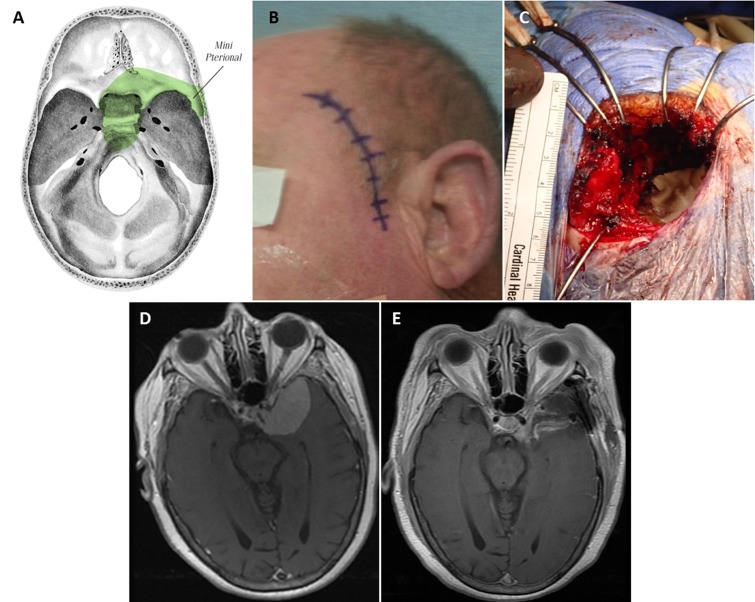
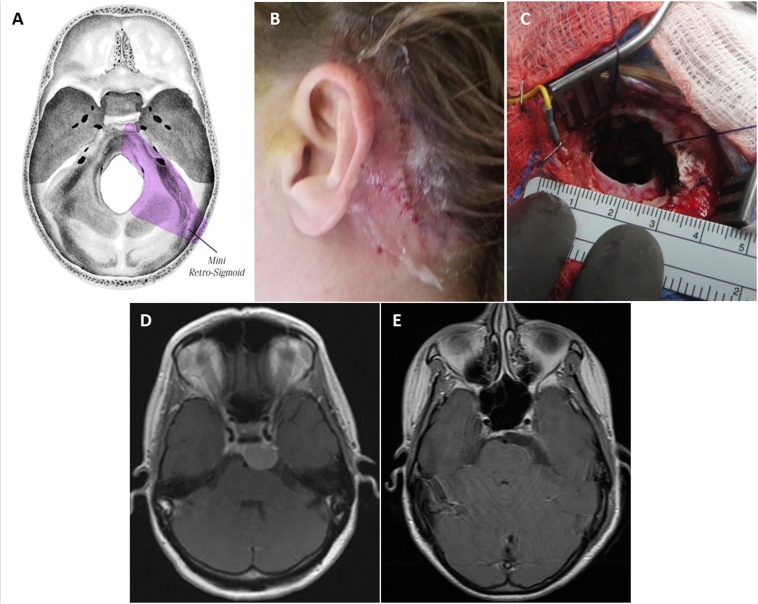
Keywords: craniotomy; eyebrow; keyhole; meningioma; pterional; retrosigmoid; supraorbital; tumor resection.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- The concept of minimally invasive neurosurgery. Teo C. Neurosurg Clin N Am. 2010;21:583–584. - PubMed
-
- The keyhole concept in neurosurgery. Reisch R, Stadie A, Kockro RA, Hopf N. World Neurosurg. 2013;79:0. - PubMed
-
- Quantitative verification of the keyhole concept: a comparison of area of exposure in the parasellar region via supraorbital keyhole, frontotemporal pterional, and supraorbital approaches. Cheng CM, Noguchi A, Dogan A, et al. J Neurosurg. 2013;118:264–269. - PubMed
-
- The supraorbital approach: technical note. Jane JA, Park TS, Pobereskin LH, Winn HR, Butler AB. Neurosurgery. 1982;11:537–542. - PubMed
-
- Ten-year experience with the supraorbital subfrontal approach through an eyebrow skin incision. Reisch R, Perneczky A. Neurosurgery. 2005;57:242–255. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources