

Endoscopic Distal Biceps Repair: Endoscopic Anatomy and Dual-Anchor Repair Using a Proximal Anterolateral "Parabiceps Portal"
- PMID: 27284512
- PMCID: PMC4886957
- DOI: 10.1016/j.eats.2015.07.031
Endoscopic Distal Biceps Repair: Endoscopic Anatomy and Dual-Anchor Repair Using a Proximal Anterolateral "Parabiceps Portal"
Abstract
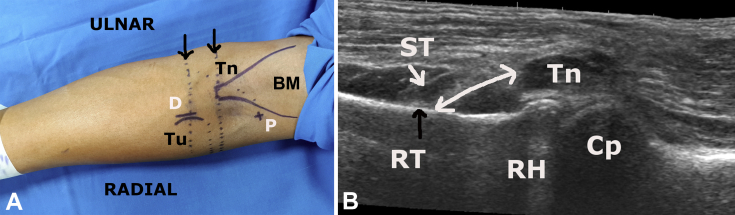
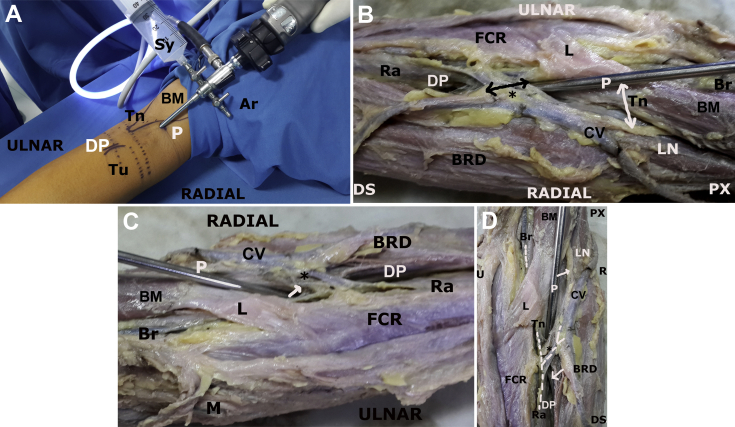
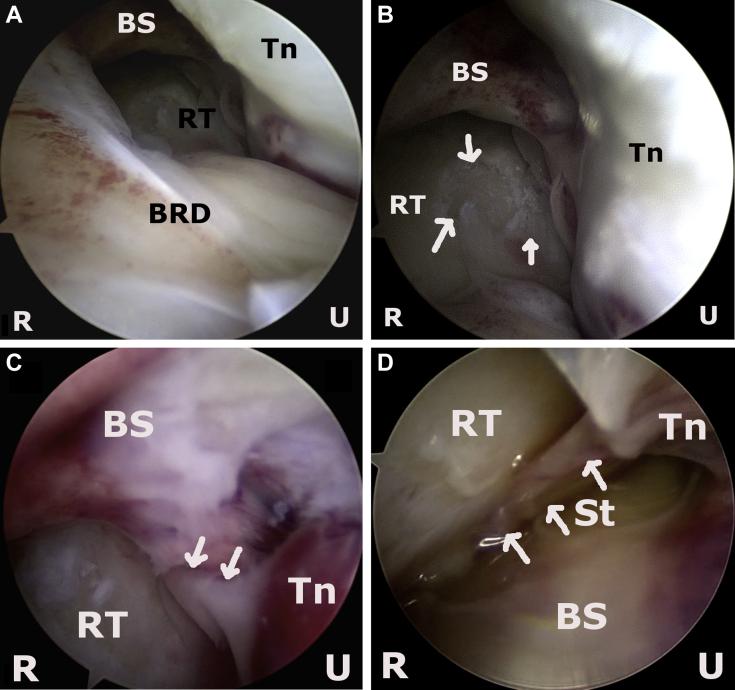
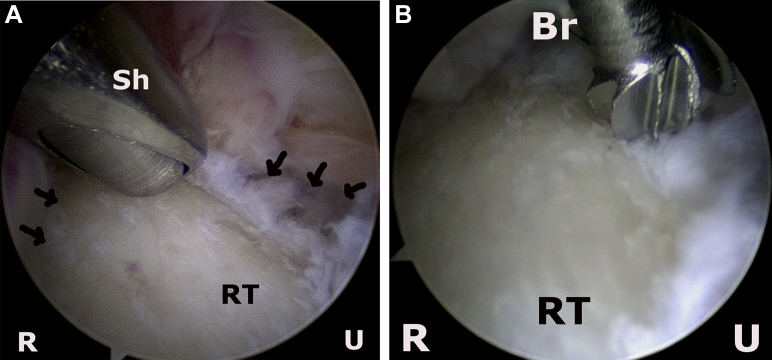
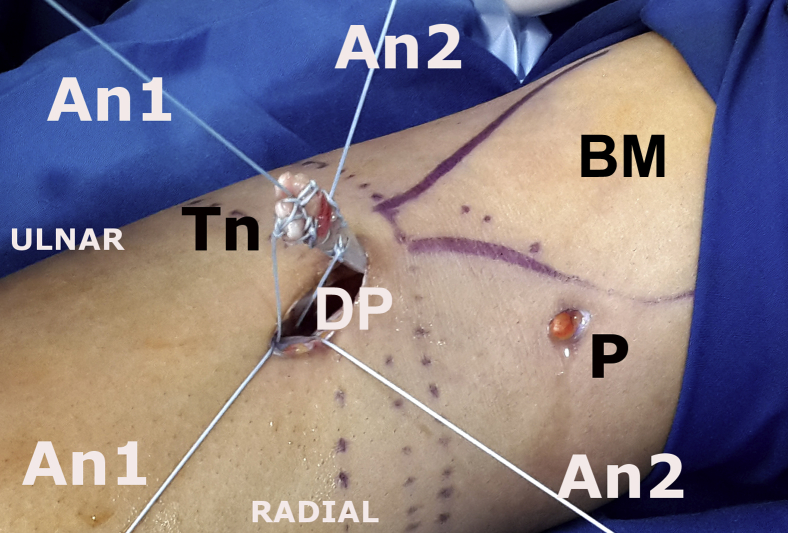
Distal biceps rupture is associated with significant functional disability, and surgical treatment involves open or endoscopic-assisted repair of the ruptured tendon through an anterior incision. This report describes an endoscopic approach that is performed with 2 portals for visualization and instrumentation. Preoperative sonography is used to identify bony and soft-tissue landmarks. The viewing portal is a proximal anterolateral "parabiceps portal" developed by the author, and the landmarks and relevant anatomic relations have been derived from a preliminary anatomic study. The working portal is a distal anterior portal and permits access to the radial tuberosity through the internervous muscular plane. The parabiceps portal permits visualization of the anterior and medial region of the radial tuberosity. A detailed description of the endoscopic pathoanatomy of the distal biceps tendon region is presented. The distal anterior portal is used for retrieval of the ruptured tendon, and thereafter the tuberosity is debrided and anchors are placed under vision. The ruptured tendon is whipstitched and docked onto the tuberosity, and nonsliding knots are used to securely reattach the tendon to bone. Overall, the 2-portal technique provides a method for tendon repair under direct visualization and is safe and reproducible.
Figures





Similar articles
-
Cadaveric study of anterior and posterior elbow endoscopy portals for endoscopic distal biceps repair: comparative anatomy-at-risk.Surg Radiol Anat. 2016 Sep;38(7):781-91. doi: 10.1007/s00276-016-1637-6. Epub 2016 Feb 9. Surg Radiol Anat. 2016. PMID: 26861011
-
Endoscopic Repair of Acute and Chronic Retracted Distal Biceps Ruptures.J Hand Surg Am. 2016 Dec;41(12):e501-e507. doi: 10.1016/j.jhsa.2016.09.008. Epub 2016 Oct 13. J Hand Surg Am. 2016. PMID: 27743752 Review.
-
Endoscopic anatomy of distal biceps tendon insertion and bicipitoradial bursa: a cadaveric study.J Shoulder Elbow Surg. 2021 Aug;30(8):1759-1767. doi: 10.1016/j.jse.2020.11.033. Epub 2021 Jan 21. J Shoulder Elbow Surg. 2021. PMID: 33486057
-
Distal Biceps Tendon Repair Using a Single Incision, Dual Anchor Technique.Video J Sports Med. 2023 Apr 11;3(2):26350254231155500. doi: 10.1177/26350254231155500. eCollection 2023 Mar-Apr. Video J Sports Med. 2023. PMID: 40309422 Free PMC article.
-
[Proximal and distal biceps tendon rupture--an indication for surgery?].Unfallchirurg. 1998 Sep;101(9):735-9. doi: 10.1007/s001130050331. Unfallchirurg. 1998. PMID: 9816985 Review. German.
Cited by
-
Cadaveric study of anterior and posterior elbow endoscopy portals for endoscopic distal biceps repair: comparative anatomy-at-risk.Surg Radiol Anat. 2016 Sep;38(7):781-91. doi: 10.1007/s00276-016-1637-6. Epub 2016 Feb 9. Surg Radiol Anat. 2016. PMID: 26861011
-
Minimally invasive distal biceps tendon repair: a case series.Clin Shoulder Elb. 2023 Sep;26(3):222-230. doi: 10.5397/cise.2023.00227. Epub 2023 Sep 1. Clin Shoulder Elb. 2023. PMID: 37652743 Free PMC article.
-
"All-Endoscopic" Management of Refractory Elbow Bicipitoradial Bursitis and Partial Distal Biceps Tendon Tears.Arthrosc Tech. 2022 May 21;11(6):e1087-e1095. doi: 10.1016/j.eats.2022.02.017. eCollection 2022 Jun. Arthrosc Tech. 2022. PMID: 35782832 Free PMC article.
References
-
- Baker B.E., Bierwagen D. Rupture of the distal tendon of the biceps brachii. Operative versus non-operative treatment. J Bone Joint Surg Am. 1985;67:414–417. - PubMed
-
- Watson J.N., Moretti V.M., Schwindel L., Hutchinson M.R. Repair techniques for acute distal biceps tendon ruptures: A systematic review. J Bone Joint Surg Am. 2014;96:2086–2090. - PubMed
-
- Phadnis J., Bain G. Endoscopic-assisted distal biceps footprint repair. Tech Hand Up Extrem Surg. 2015;19:55–59. - PubMed
-
- Greenberg J.A., Fernandez J.J., Wang T. EndoButton-assisted repair of distal biceps tendon ruptures. J Shoulder Elbow Surg. 2003;12:484–490. - PubMed
-
- Grégory T., Roure P., Fontès D. Repair of distal biceps tendon rupture using a suture anchor: Description of a new endoscopic procedure. Am J Sports Med. 2009;37:506–511. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
