

Clinically important improvement thresholds for Harris Hip Score and its ability to predict revision risk after primary total hip arthroplasty
- PMID: 27286675
- PMCID: PMC4901425
- DOI: 10.1186/s12891-016-1106-8
Clinically important improvement thresholds for Harris Hip Score and its ability to predict revision risk after primary total hip arthroplasty
Abstract
Background: Some aspects of validity are missing for the Harris Hip Score (HHS). Our objective was to examine the clinically meaningful change thresholds, responsiveness and the predictive ability of the HHS questionnaire.
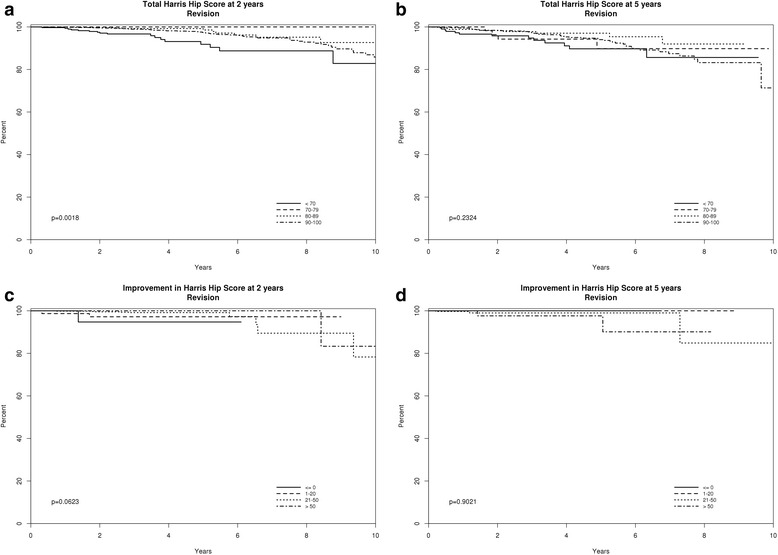
Methods: We included a cohort of patients who underwent primary total hip arthroplasty (THA) and responded to the HHS preoperatively and at 2- or 5-year post-THA (change score) to examine the clinically meaningful change thresholds (Minimal clinically important improvement, MCII; and moderate improvement), responsiveness (effect size (ES) and standardized response mean (SRM)) based on pre- to post-operative change and the predictive ability of change score or absolute postoperative score at 2- and 5-years post-THA for future revision.
Results: Two thousand six hundred sixty-seven patients with a mean age of 64 years completed baseline HHS; 1036 completed both baseline and 2-year HHS and 669 both baseline and 5-year HHS. MCII and moderate improvement thresholds ranged 15.9-18 points and 39.6-40.1 points, respectively. ES was 3.12 and 3.02 at 2- and 5-years; respective SRM was 2.73 and 2.52. There were 3195 hips with HHS scores at 2-years and 2699 hips with HHS scores at 5-years (regardless of the completion of baseline HHS; absolute postoperative scores). Compared to patients with absolute HHS scores of 81-100 (score range, 0-100), patients with scores <55 at 2- and 5-years had higher hazards (95 % confidence interval) of subsequent revision, 4.34 (2.14, 7.95; p < 0.001) and 3.08 (1.45, 5.84; p = 0.002), respectively. Compared to HHS score improvement of >50 points from preoperative to 2-years post-THA, lack of improvement/worsening or 1-20 point improvement were associated with increased hazards of revision, 18.10 (1.41, 234.83; p = 0.02); and 6.21 (0.81, 60.73; p = 0.10), respectively.
Conclusions: HHS is a valid measure of THA outcomes and is responsive to change. Both absolute HHS postoperative scores and HHS score change postoperatively are predictive of revision risk post-primary THA. We defined MCID and moderate improvement thresholds for HHS in this study.
Keywords: Clinically important improvement; Discriminant ability; Harris Hip Score; MCID; MCII; Minimal clinically important difference; Minimal clinically important improvement; Predictability; Responsiveness; Total Hip Arthroplasty.
Figures

References
-
- Healthcare Cost and Utilization Project (HCUP). HCUP Facts and Figures 2009- Section 3: Inpatient Hospital Stays by Procedure. Exhibit 3.1 Most Frequent All-listed Procedures. http://hcup-us.ahrq.gov/reports/factsandfigures/2009/pdfs/FF_2009_sectio.... Accessed 3 June 2016.
-
- Report to the Chairman, Committee on Finance, U.S. Senate. Medicare. Lack of Price Transparency May Hamper Hospitals’ Ability to Be Prudent Purchasers of Implantable Medical Devices. GAO-12-126. http://www.gao.gov/assets/590/587688.pdf. Accessed 3 June 2016.
-
- Harris WH. Traumatic arthritis of the hip after dislocation and acetabular fractures: treatment by mold arthroplasty. An end-result study using a new method of result evaluation. J Bone Joint Surg Am. 1969;51(4):737–55. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
