

Definition by FSH, AMH and embryo numbers of good-, intermediate- and poor-prognosis patients suggests previously unknown IVF outcome-determining factor associated with AMH
- PMID: 27286817
- PMCID: PMC4901433
- DOI: 10.1186/s12967-016-0924-7
Definition by FSH, AMH and embryo numbers of good-, intermediate- and poor-prognosis patients suggests previously unknown IVF outcome-determining factor associated with AMH
Abstract
Background: Though outcome models have been proposed previously, it is unknown whether cutoffs in clinical pregnancy and live birth rates at all ages are able to classify in vitro fertilization (IVF) patients into good-, intermediate- and poor prognosis.
Methods: We here in 3 infertile patient cohorts, involving 1247, 1514 and 632 women, built logistic regression models based on 3 functional ovarian reserve (FOR) parameters, including (1) number of good quality embryos, (2) follicle stimulating hormone (FSH, mIU/mL) and (3) anti-Müllerian hormone (AMH, ng/mL), determining whether clinical pregnancy and live birth rates can discriminate between good, intermediate and poor prognosis patients.
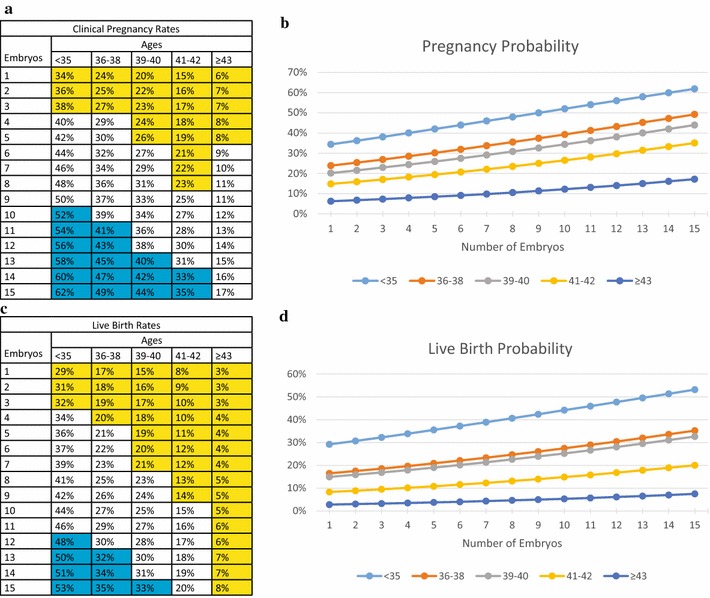
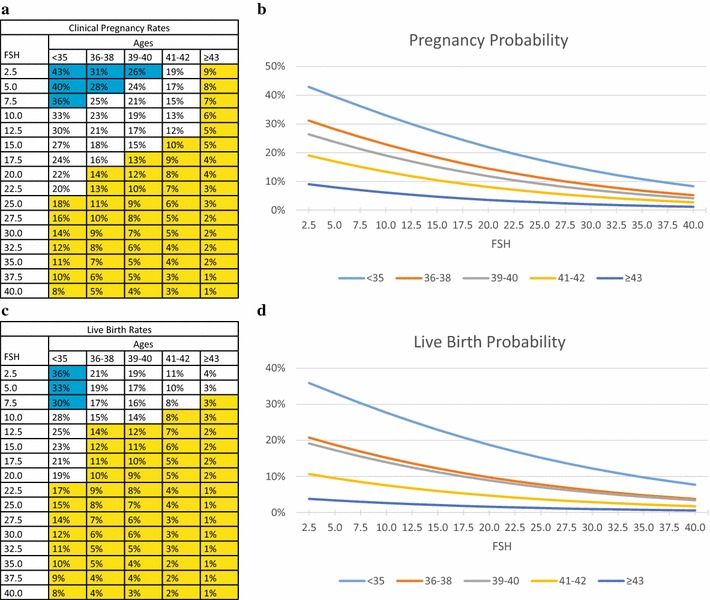
Results: All models, indeed, allowed at all ages for separation by prognosis, though cut offs changed with age. In the embryo model, increasing embryo production resulted in linear improvement of IVF outcomes despite transfer of similar embryo numbers; in the FSH model outcomes and FSH levels related inversely, while the association of AMH followed a bell-shaped polynomial pattern, demonstrating "best" outcomes at mid-ranges. All 3 models demonstrated increasingly poor outcomes with advancing ages, though "best" AMH even above age 43 was still associated with unexpectedly good pregnancy and delivery outcomes. Excessively high AMH, in contrast, was at all ages associated with spiking miscarriage rates.
Conclusions: At varying peripheral serum concentrations, AMH, thus, demonstrates hithero unknown and contradictory effects on IVF outcomes, deserving at different concentrations investigation as a potential therapeutic agent, with pregnancy-supporting and pregnancy-interrupting properties.
Keywords: Anti-Müllerian hormone (AMH); Embryo number; Follicle stimulating hormone (FSH); In vitro fertilization (IVF); Live birth rates; Prediction models; Prognosis.
Figures

Similar articles
-
Discordant anti-müllerian hormone (AMH) and follicle stimulating hormone (FSH) among women undergoing in vitro fertilization (IVF): which one is the better predictor for live birth?J Ovarian Res. 2018 Jul 16;11(1):60. doi: 10.1186/s13048-018-0430-z. J Ovarian Res. 2018. PMID: 30012195 Free PMC article.
-
How FSH and AMH reflect probabilities of oocyte numbers in poor prognosis patients with small oocyte yields.Endocrine. 2016 Nov;54(2):476-483. doi: 10.1007/s12020-016-1068-5. Epub 2016 Aug 10. Endocrine. 2016. PMID: 27510172
-
Maternal serum concentration of anti-Müllerian hormone is a better predictor than basal follicle stimulating hormone of successful blastocysts development during IVF treatment.PLoS One. 2020 Oct 12;15(10):e0239779. doi: 10.1371/journal.pone.0239779. eCollection 2020. PLoS One. 2020. PMID: 33044971 Free PMC article.
-
Making IVF more effective through the evolution of prediction models: is prognosis the missing piece of the puzzle?Syst Biol Reprod Med. 2018 Oct;64(5):305-323. doi: 10.1080/19396368.2018.1504347. Epub 2018 Aug 8. Syst Biol Reprod Med. 2018. PMID: 30088950 Review.
-
Is the measurement of anti-Müllerian hormone essential?Curr Opin Obstet Gynecol. 2012 Jun;24(3):151-7. doi: 10.1097/GCO.0b013e3283527dcf. Curr Opin Obstet Gynecol. 2012. PMID: 22487725 Review.
Cited by
-
Effect of different combinations of serum antimüllerian hormone levels and body mass index on pregnancy outcomes in women with polycystic ovary syndrome.AJOG Glob Rep. 2025 Feb 22;5(2):100461. doi: 10.1016/j.xagr.2025.100461. eCollection 2025 May. AJOG Glob Rep. 2025. PMID: 40162007 Free PMC article.
-
Stress, anxiety, and depression in infertile couples are not associated with a first IVF or ICSI treatment outcome.BMC Pregnancy Childbirth. 2021 Oct 27;21(1):725. doi: 10.1186/s12884-021-04202-9. BMC Pregnancy Childbirth. 2021. PMID: 34706683 Free PMC article.
-
An additive opinion to the committee opinion of ASRM and SART on the use of preimplantation genetic testing for aneuploidy (PGT-A).J Assist Reprod Genet. 2025 Jan;42(1):71-80. doi: 10.1007/s10815-024-03318-z. Epub 2024 Dec 18. J Assist Reprod Genet. 2025. PMID: 39693036
-
Anti-Müllerian hormone treatment enhances oocyte quality, embryonic development and live birth rate†.Biol Reprod. 2022 Sep 12;107(3):813-822. doi: 10.1093/biolre/ioac116. Biol Reprod. 2022. PMID: 35657015 Free PMC article.
-
IVF outcomes of women with discrepancies between age and serum anti-Müllerian hormone levels.Reprod Biol Endocrinol. 2019 Jul 16;17(1):58. doi: 10.1186/s12958-019-0498-3. Reprod Biol Endocrinol. 2019. PMID: 31311571 Free PMC article.
References
-
- Fertility Clinic Success Rate and Certification Act of 1992. HR 4773ENR.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
