

Origin, Clinical Characteristics and 30-Day Outcomes of Severe Hematochezia in Cirrhotics and Non-cirrhotics
- PMID: 27286877
- PMCID: PMC5602600
- DOI: 10.1007/s10620-016-4198-y
Origin, Clinical Characteristics and 30-Day Outcomes of Severe Hematochezia in Cirrhotics and Non-cirrhotics
Abstract
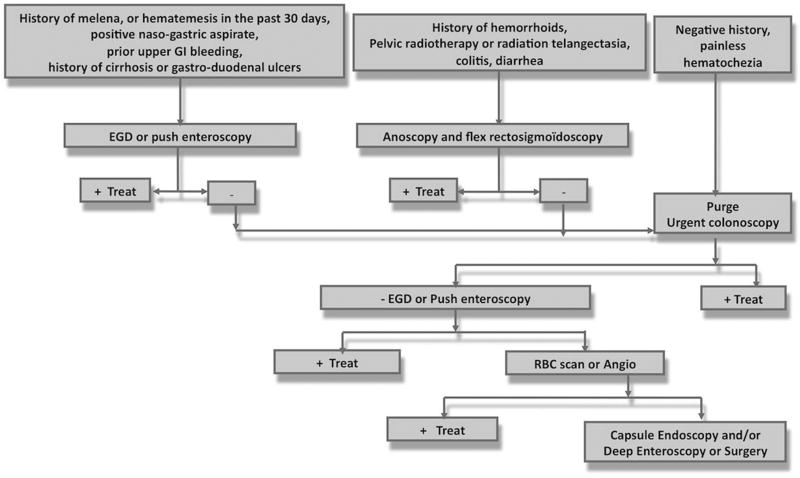
Background: The sites of origin, causes and outcomes of severe hematochezia have not been compared between cirrhotics and non-cirrhotics. In cirrhotics versus non-cirrhotics presenting with severe hematochezia, we aimed at (1) identifying the site and etiology of gastro-intestinal bleeding and independent predictors of bleeding from the upper gastrointestinal tract versus small bowel or the colon, (2) comparing 30-day clinical outcomes, and (3) proposing an algorithm for management of severe hematochezia.
Methods: In this cohort study from two university-based medical centers, 860 consecutive patients with severe hematochezia admitted from 1995 to 2011 were prospectively enrolled with 160 (18.6 %) cirrhotics. We studied (a) general clinical and laboratory characteristics of cirrhotics versus non-cirrhotics, (b) predictors of bleeding sites in each patient group by multiple variable regression analysis, and compared (c) 30-day outcomes, including rebleeding, surgery and deaths.
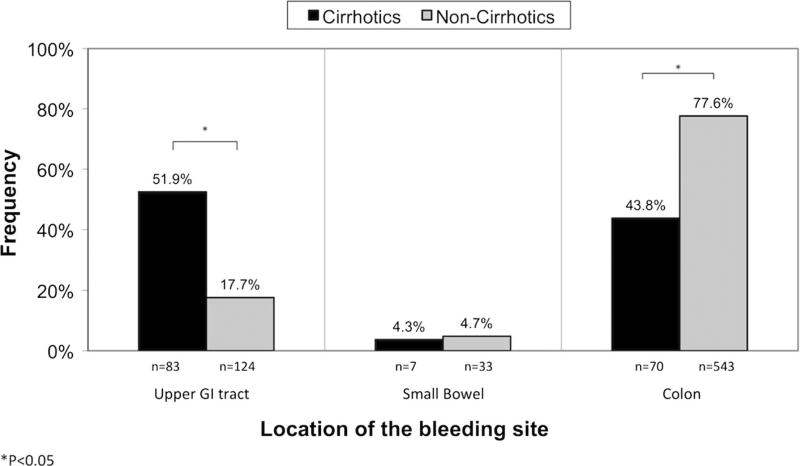
Results: Cirrhosis independently predicted an upper gastrointestinal source of bleeding (OR 3.47; 95 % CI 2.01-5.96) as well as history of hematemesis, melena in the past 30 days, positive nasogastric aspirate, prior upper gastrointestinal bleeding or use of aspirin or non-steroidal anti-inflammatory. The most prevalent diagnoses were esophageal varices (20 %) in cirrhotics and colon diverticular bleeding (27.1 %) in non-cirrhotics. Thirty-day rates of rebleeding, surgical interventions and deaths were 23.1 versus 15 % (P = 0.01), 14.4 versus 6.4 % (P < 0.001), and 17.5 versus 4.1 % (P < 0.001), in cirrhotics versus non-cirrhotics, respectively.
Conclusions: Cirrhosis predicted an upper gastrointestinal site of bleeding in patients presenting with severe hematochezia. The 30-day rates of rebleeding, surgery, and death were significantly higher in cirrhotics than in non-cirrhotics.
Keywords: Cirrhosis; Hematochezia; Lower gastrointestinal bleeding; Upper gastrointestinal bleeding.
Conflict of interest statement
Figures
References
-
- Davila RE, Rajan E, Adler DG, et al. ASGE guideline: the role of endoscopy in the patient with lower-GI bleeding. Gastrointest Endosc. 2005;62:656–660. - PubMed
-
- Zuccaro G., Jr Management of the adult patient with acute lower gastrointestinal bleeding. American College of Gastroenterology. Practice Parameters Committee. Am J Gastroenterol. 1998;93:1202–1208. - PubMed
-
- Savides TJ, Jensen DM. GI bleeding. In: Feldman M, Friedman LS, Brandt LJ, editors. Sleisenger and Fordtran’s Gastrointestinal and Liver Disease: Pathophysiology/Diagnosis/Management. 10. Philadelphia: Saunders Elsevier Saunders; 2016. pp. 297–335.
-
- Jensen DM. Management of patients with severe hematochezia—with all current evidence available. Am J Gastroenterol. 2005;100:2403–2406. - PubMed
-
- González-González JA, García-Compean D, Vázquez-Elizondo G, Garza-Galindo A, Jáquez-Quintana JO, Maldonado-Garza H. Nonvariceal upper gastrointestinal bleeding in patients with liver cirrhosis. Clinical features, outcomes and predictors of in-hospital mortality. A prospective study. Ann Hepatol. 2011;10:287–295. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
