

Desmoid-type fibromatosis of the head and neck in children: a case report and review of the literature
- PMID: 27286970
- PMCID: PMC4902910
- DOI: 10.1186/s13256-016-0949-9
Desmoid-type fibromatosis of the head and neck in children: a case report and review of the literature
Abstract
Background: Desmoid-type fibromatosis is defined as an intermediate tumor that rarely occurs in the head and neck of children. There is no doubt as to the value of complete surgical excision for desmoid-type fibromatosis. However, in pediatric patients, surgeons may often be concerned about making a wide excision because of the potential for functional morbidity. Some studies have reported a lack of correlation between margin status and recurrence. Therefore, we discussed our findings with a focus on the state of surgical margins.
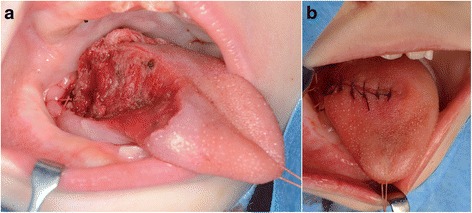
Case presentation: We report an unusual case of a 9-month-old Japanese girl who prior to presenting at our hospital underwent debulking surgery twice with chemotherapy for desmoid-type fibromatosis of the tongue at another hospital. We performed a partial glossectomy and simultaneous reconstruction with local flap and achieved microscopic complete resection. We also reviewed available literature of pediatric desmoid-type fibromatosis in the head and neck.
Conclusions: We described successful treatment for the refractory case of pediatric desmoid-type fibromatosis. The review results showed that some microscopic incomplete resections of tumors in pediatric patients with desmoid-type fibromatosis tended to be acceptable with surgical treatment.
Keywords: Case report; Children; Decision-making; Desmoid; Fibromatosis; Head and neck; Tongue.
Figures




References
-
- Barnes L, Eveson JW, Reichart P, Sidransky D. World Health Organization classification of tumors. Pathology and genetics of head and neck tumors. Lyon: IARC; 2005.
-
- Tse GM, Chan KF, Ahuja AT, King AD, Pang PC, To EW. Fibromatosis of the head and neck region. Otolaryngol Head Neck Surg. 2001;125:516–9. - PubMed
-
- Kasper B, Baumgarten C, Bonvalot S, et al. Management of sporadic desmoid-type fibromatosis: a European consensus approach based on patients’ and professionals’ expertise – a sarcoma patients EuroNet and European Organisation for Research and Treatment of Cancer/Soft Tissue and Bone Sarcoma Group initiative. Eur J Cancer. 2015;51:127–36. doi: 10.1016/j.ejca.2014.11.005. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
