

Quantification of risk factors for postherpetic neuralgia in herpes zoster patients: A cohort study
- PMID: 27287218
- PMCID: PMC4932239
- DOI: 10.1212/WNL.0000000000002808
Quantification of risk factors for postherpetic neuralgia in herpes zoster patients: A cohort study
Abstract
Objective: To investigate risk factors for postherpetic neuralgia, the neuropathic pain that commonly follows herpes zoster.
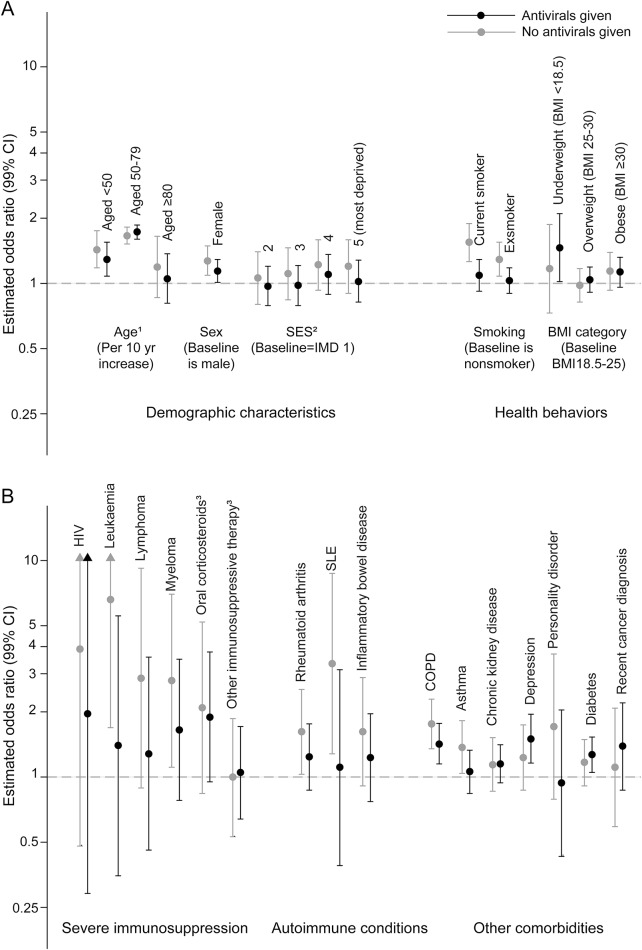
Methods: Using primary care data from the Clinical Practice Research Datalink, we fitted multivariable logistic regression models to investigate potential risk factors for postherpetic neuralgia (defined as pain ≥90 days after zoster, based on diagnostic or prescription codes), including demographic characteristics, comorbidities, and characteristics of the acute zoster episode. We also assessed whether the effects were modified by antiviral use.
Results: Of 119,413 zoster patients, 6,956 (5.8%) developed postherpetic neuralgia. Postherpetic neuralgia risk rose steeply with age, most sharply between 50 and 79 years (adjusted odds ratio [OR] for a 10-year increase, 1.70, 99% confidence interval 1.63-1.78). Postherpetic neuralgia risk was higher in women (6.3% vs 5.1% in men: OR 1.19, 1.10-1.27) and those with severely immunosuppressive conditions, including leukemia (13.7%: 2.07, 1.08-3.96) and lymphoma (12.7%: 2.45, 1.53-3.92); autoimmune conditions, including rheumatoid arthritis (9.1%: 1.20, 0.99-1.46); and other comorbidities, including asthma and diabetes. Current and ex-smokers, as well as underweight and obese individuals, were at increased risk of postherpetic neuralgia. Antiviral use was not associated with postherpetic neuralgia (OR 1.04, 0.97-1.11). However, the increased risk associated with severe immunosuppression appeared less pronounced in patients given antivirals.
Conclusions: Postherpetic neuralgia risk was increased for a number of patient characteristics and comorbidities, notably with age and among those with severe immunosuppression. As zoster vaccination is contraindicated for patients with severe immunosuppression, strategies to prevent zoster in these patients, which could include the new subunit zoster vaccine, are an increasing priority.
© 2016 American Academy of Neurology.
Figures
References
-
- Dworkin RH, Schmader KE, Goldstein EJC. Treatment and prevention of postherpetic neuralgia. Clin Infect Dis 2003;36:877–882. - PubMed
-
- Weaver BA. The burden of herpes zoster and postherpetic neuralgia in the United States. J Am Osteopath Assoc 2007;107(suppl 1):S2–S7. - PubMed
-
- Thomas SL, Hall AJ. What does epidemiology tell us about risk factors for herpes zoster? Lancet Infect Dis 2004;4:26–33. - PubMed
-
- Sacks GM. Unmet need in the treatment of postherpetic neuralgia. Am J Manag Care 2013;19(1 suppl):S207–S213. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials