

New chemosensory component in the U.S. National Health and Nutrition Examination Survey (NHANES): first-year results for measured olfactory dysfunction
- PMID: 27287364
- PMCID: PMC5033684
- DOI: 10.1007/s11154-016-9364-1
New chemosensory component in the U.S. National Health and Nutrition Examination Survey (NHANES): first-year results for measured olfactory dysfunction
Abstract
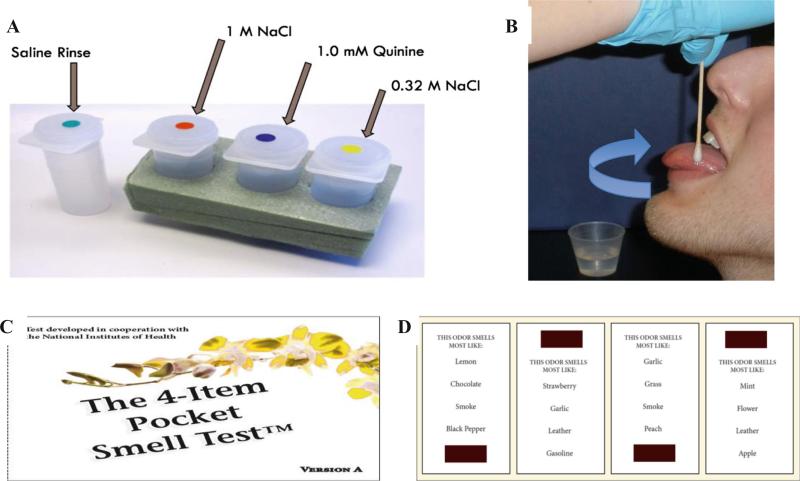
The U.S. NHANES included chemosensory assessments in the 2011-2014 protocol. We provide an overview of this protocol and 2012 olfactory exam findings. Of the 1818 NHANES participants aged ≥40 years, 1281 (70.5 %) completed the exam; non-participation mostly was due to time constraints. Health technicians administered an 8-item, forced-choice, odor identification task scored as normosmic (6-8 odors identified correctly) versus olfactory dysfunction, including hyposmic (4-5 correct) and anosmic/severe hyposmic (0-3 correct). Interviewers recorded self-reported smell alterations (during past year, since age 25, phantosmia), histories of sinonasal problems, xerostomia, dental extractions, head or facial trauma, and chemosensory-related treatment and changes in quality of life. Olfactory dysfunction was found in 12.4 % (13.3 million adults; 55 % males/45 % females) including 3.2 % anosmic/severe hyposmic (3.4 million; 74 % males/26 % females). Selected age-specific prevalences were 4.2 % (40-49 years), 12.7 % (60-69 years), and 39.4 % (80+ years). Among adults ≥70 years, misidentification rates for warning odors were 20.3 % for smoke and 31.3 % for natural gas. The highest sensitivity (correctly identifying dysfunction) and specificity (correctly identifying normosmia) of self-reported olfactory alteration was among anosmics/severe hyposmics (54.4 % and 78.1 %, respectively). In age- and sex-adjusted logistic regression analysis, risk factors of olfactory dysfunction were racial/ethnic minority, income-to-poverty ratio ≤ 1.1, education <high school, and heavy drinking. Moderate-to-vigorous physical activity reduced risk of impairment. Olfactory dysfunction is prevalent, particularly among older adults. Inexpensive, brief odor identification tests coupled with questions (smell problems past year, since age 25, phantosmia) could screen for marked dysfunction. Healthcare providers should be prepared to offer education on non-olfactory avoidance of hazardous events.
Keywords: Epidemiology; Health status; Olfaction disorders; Public health surveillance; Risk factors; Taste.
Figures
References
-
- Centers for Disease Control and Prevention (CDC) National Center for Health Statistics (NCHS) [May 20, 2016];National Health and Nutrition Examination Survey: Plan and Operations, 1999–2010. Available from: http://www.cdc.gov/nchs/data/series/sr_01/sr01_056.pdf.
-
- National Institutes on Deafness and Other Communication Disorders [May 20, 2016];NIDCD Workshop on Epidemiology of Communication Disorders. 2005 Available from: http://www.nidcd.nih.gov/funding/programs/pages/episummary.aspx.
-
- U.S. Department of Health and Human Services. Office of Disease Prevention and Health Promotion [May 20, 2016];Healthy People 2020 Topics & Objectives: Hearing and Other Sensory or Communication Disorders. Available from: http://www.healthypeople.gov/2020/topicsobjectives2020/objectiveslist.as....
-
- CDC. NCHS [May 20, 2016];National Health and Nutrition Examination Survey (NHANES) Taste and Smell Examination Component Manual. Available from: http://www.cdc.gov/nchs/data/nhanes/nhanes_13_14/Taste_Smell.pdf.
-
- NIH Blueprint for Neuroscience Research [May 20, 2016];NIH Toolbox For the Assessment of Neurological and Behavioral Function. Available from: http://www.nihtoolbox.org/WhatAndWhy/Sensation.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
