

Krüppel-Like Factor 15 Mediates Glucocorticoid-Induced Restoration of Podocyte Differentiation Markers
- PMID: 27288011
- PMCID: PMC5198263
- DOI: 10.1681/ASN.2015060672
Krüppel-Like Factor 15 Mediates Glucocorticoid-Induced Restoration of Podocyte Differentiation Markers
Abstract
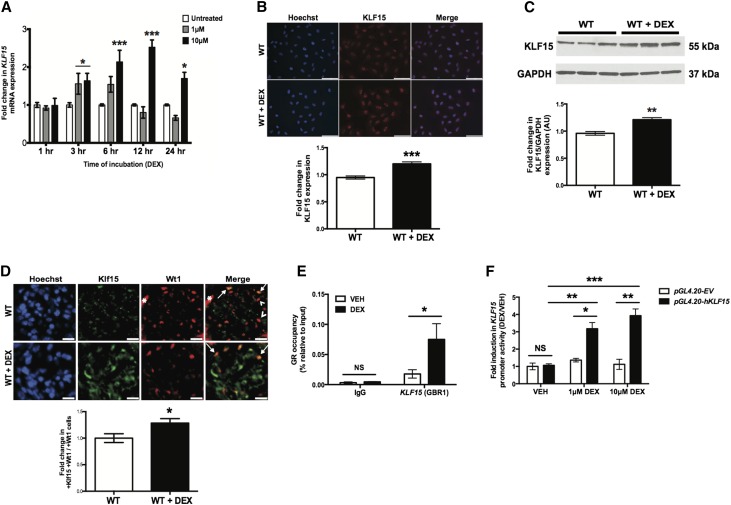
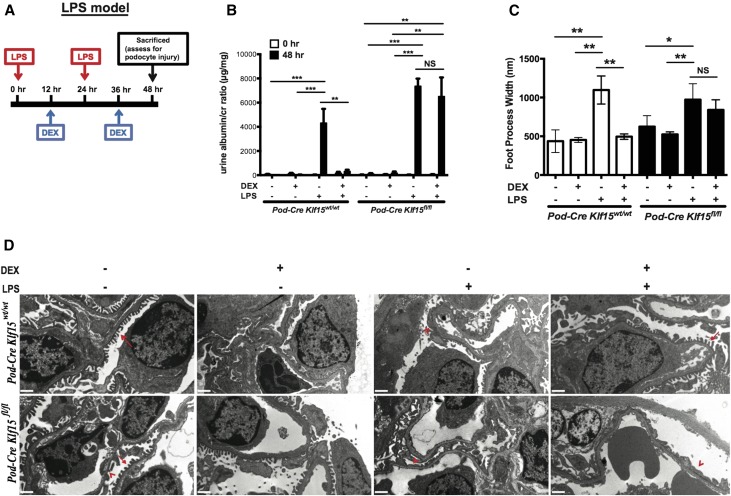
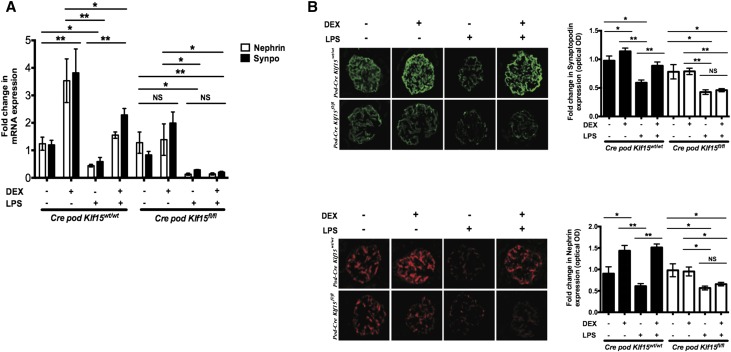
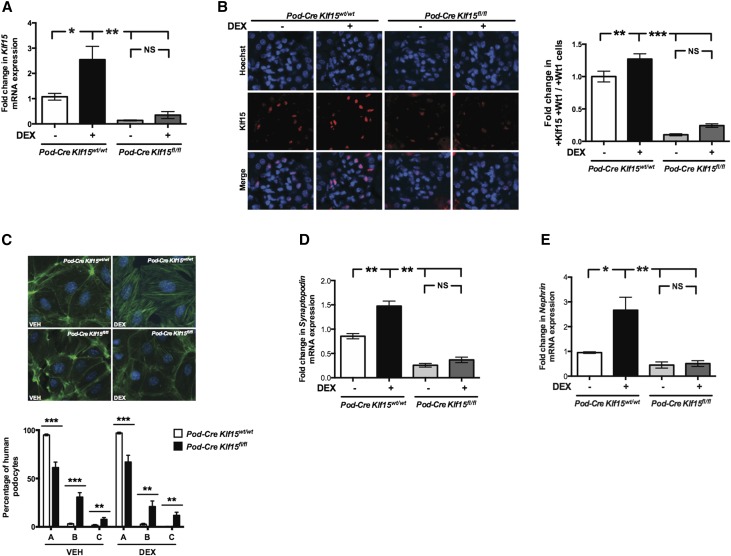
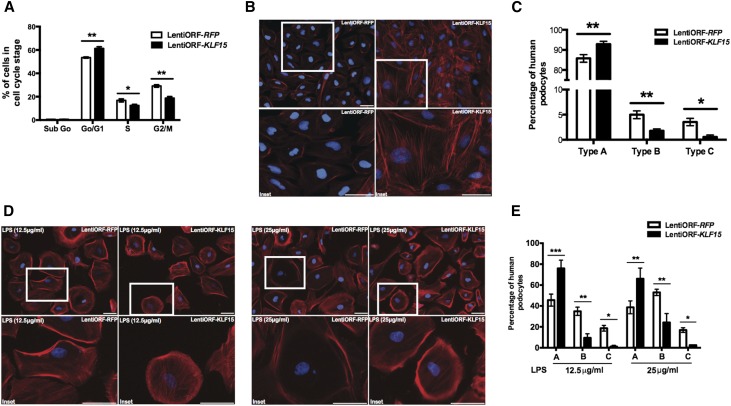
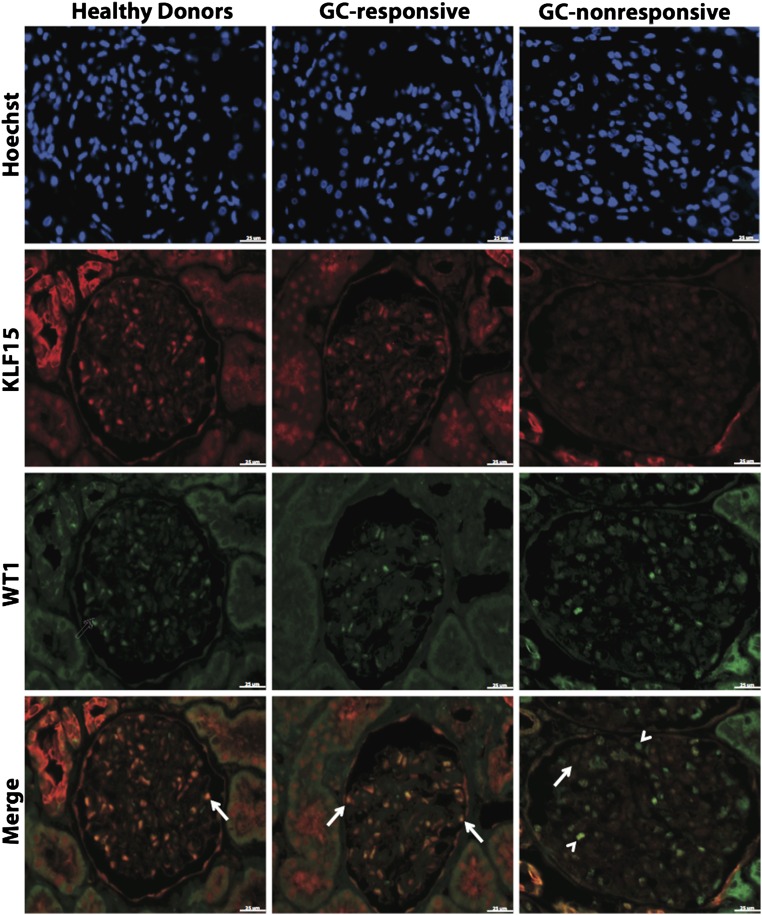
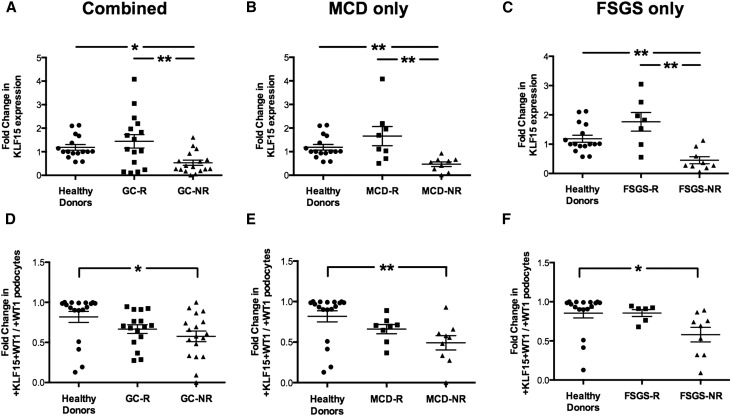
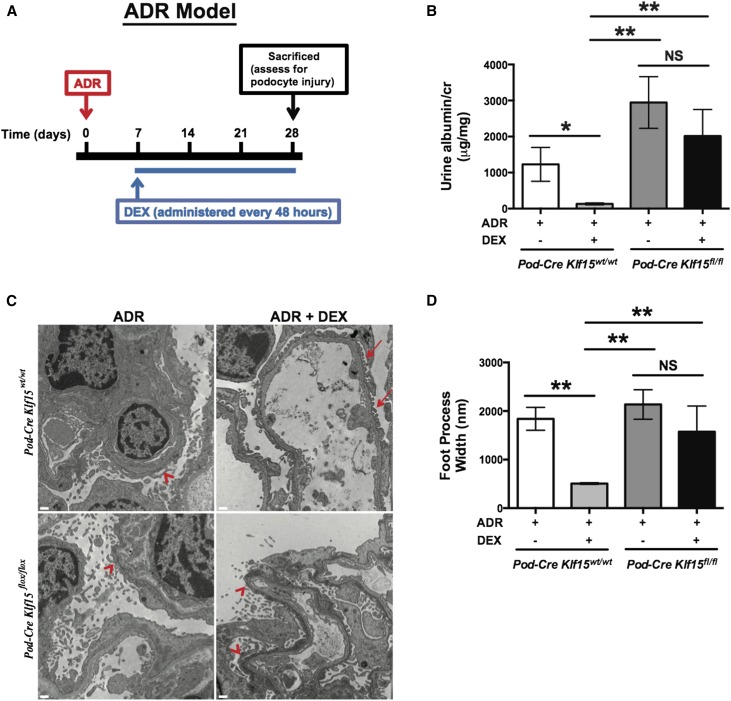
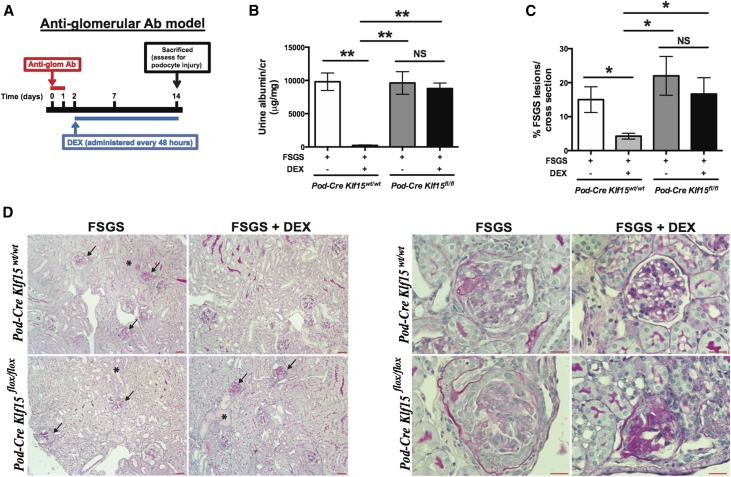
Podocyte injury is the inciting event in primary glomerulopathies, such as minimal change disease and primary FSGS, and glucocorticoids remain the initial and often, the primary treatment of choice for these glomerulopathies. Because inflammation is not readily apparent in these diseases, understanding the direct effects of glucocorticoids on the podocyte, independent of the immunomodulatory effects, may lead to the identification of targets downstream of glucocorticoids that minimize toxicity without compromising efficacy. Several studies showed that treatment with glucocorticoids restores podocyte differentiation markers and normal ultrastructure and improves cell survival in murine podocytes. We previously determined that Krüppel-like factor 15 (KLF15), a kidney-enriched zinc finger transcription factor, is required for restoring podocyte differentiation markers in mice and human podocytes under cell stress. Here, we show that in vitro treatment with dexamethasone induced a rapid increase of KLF15 expression in human and murine podocytes and enhanced the affinity of glucocorticoid receptor binding to the promoter region of KLF15 In three independent proteinuric murine models, podocyte-specific loss of Klf15 abrogated dexamethasone-induced podocyte recovery. Furthermore, knockdown of KLF15 reduced cell survival and destabilized the actin cytoskeleton in differentiated human podocytes. Conversely, overexpression of KLF15 stabilized the actin cytoskeleton under cell stress in human podocytes. Finally, the level of KLF15 expression in the podocytes and glomeruli from human biopsy specimens correlated with glucocorticoid responsiveness in 35 patients with minimal change disease or primary FSGS. Thus, these studies identify the critical role of KLF15 in mediating the salutary effects of glucocorticoids in the podocyte.
Keywords: focal segmental glomerulosclerosis; glucocorticoid; minimal change disease; podocyte.
Copyright © 2016 by the American Society of Nephrology.
Figures
References
-
- Wiggins RC: The spectrum of podocytopathies: A unifying view of glomerular diseases. Kidney Int 71: 1205–1214, 2007 - PubMed
-
- Meyrier A: Mechanisms of disease: Focal segmental glomerulosclerosis. Nat Clin Pract Nephrol 1: 44–54, 2005 - PubMed
-
- Barisoni L: Podocyte biology in segmental sclerosis and progressive glomerular injury. Adv Chronic Kidney Dis 19: 76–83, 2012 - PubMed
-
- Barnes PJ: Anti-inflammatory actions of glucocorticoids: Molecular mechanisms. Clin Sci (Lond) 94: 557–572, 1998 - PubMed
-
- Riccardi C, Bruscoli S, Migliorati G: Molecular mechanisms of immunomodulatory activity of glucocorticoids. Pharmacol Res 45: 361–368, 2002 - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
