

Pancreatic stellate cells regulate blood vessel density in the stroma of pancreatic ductal adenocarcinoma
- PMID: 27288147
- PMCID: PMC5123629
- DOI: 10.1016/j.pan.2016.05.393
Pancreatic stellate cells regulate blood vessel density in the stroma of pancreatic ductal adenocarcinoma
Abstract
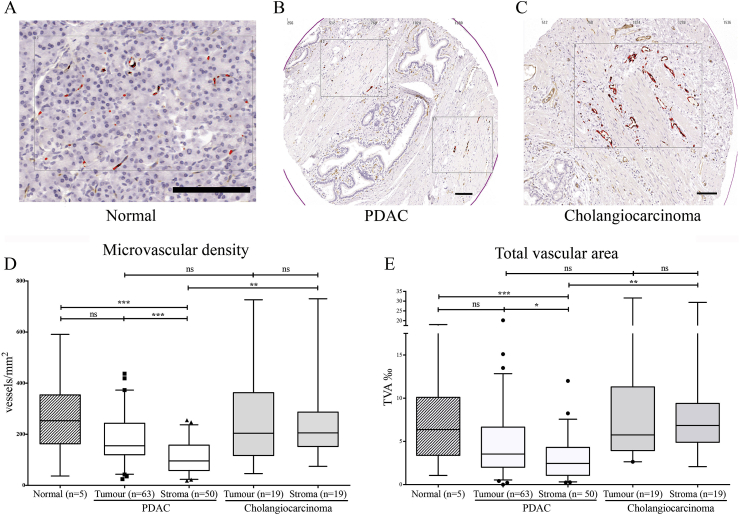
Background/objectives: The vascular heterogeneity of pancreatic ductal adenocarcinoma (PDAC) has never been characterised. We analysed the heterogeneous vascular density of human PDAC along with its prognostic correlation.
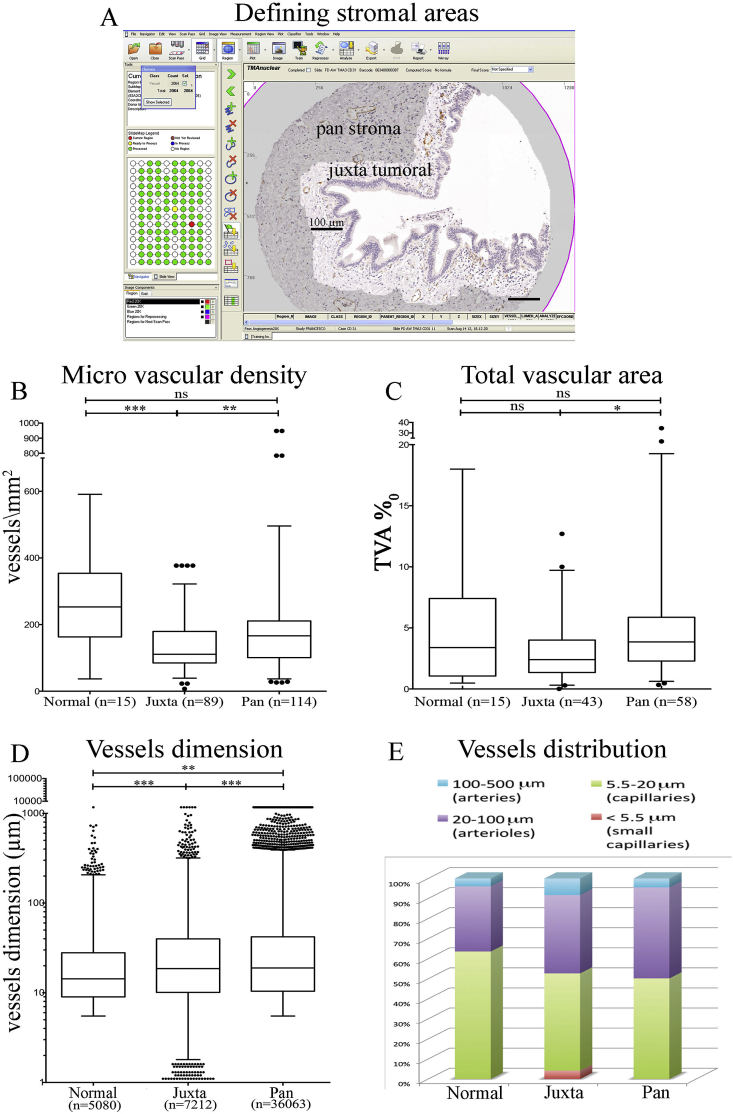
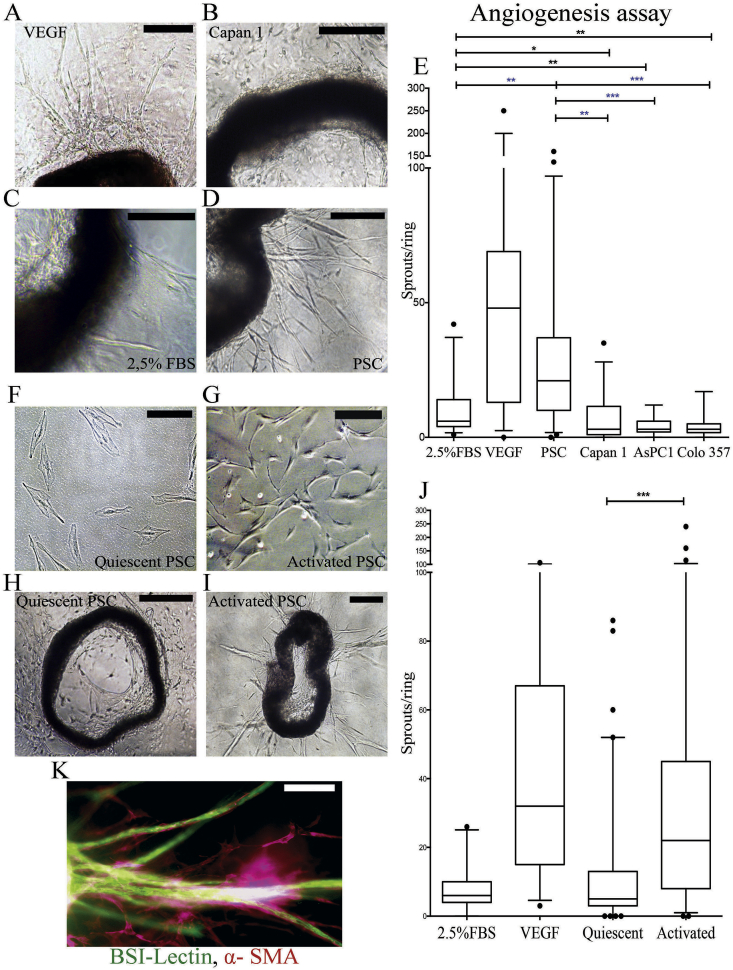
Methods: Tissue Microarrays of 87 patients with different pancreatico-biliary pathologies were analysed in an automated manner (Ariol™) after CD31 staining to assess vascular density in juxta-tumoral and panstromal compartments. In vitro and ex vivo assays were carried out to assess the role of PSC.
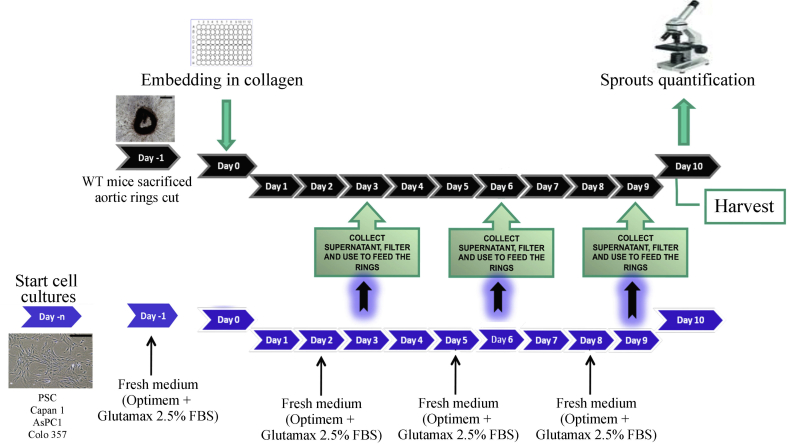
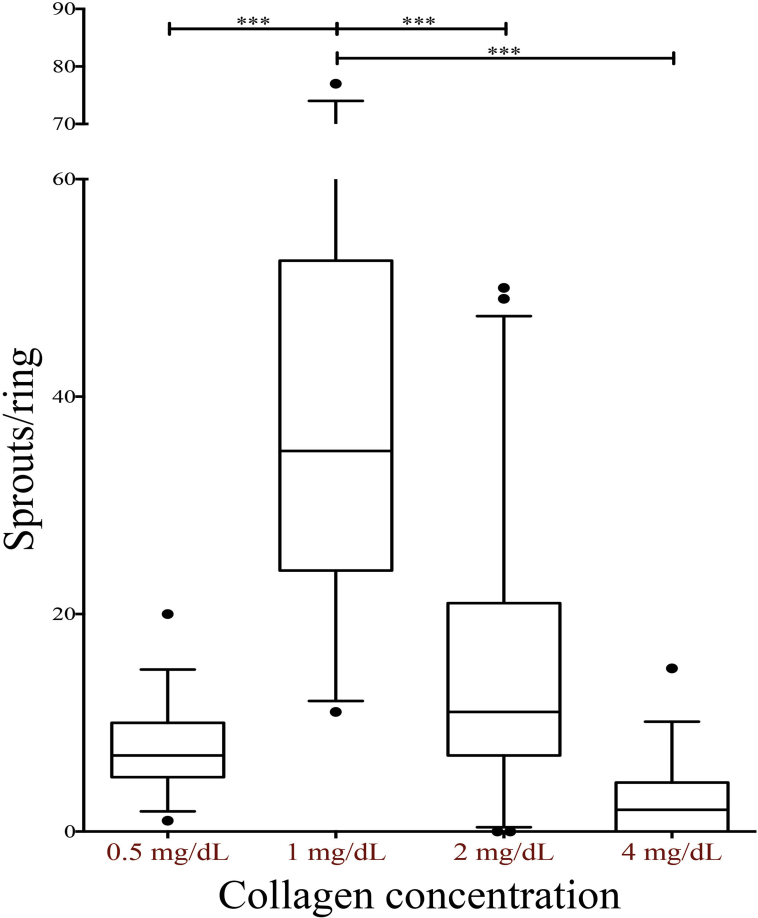
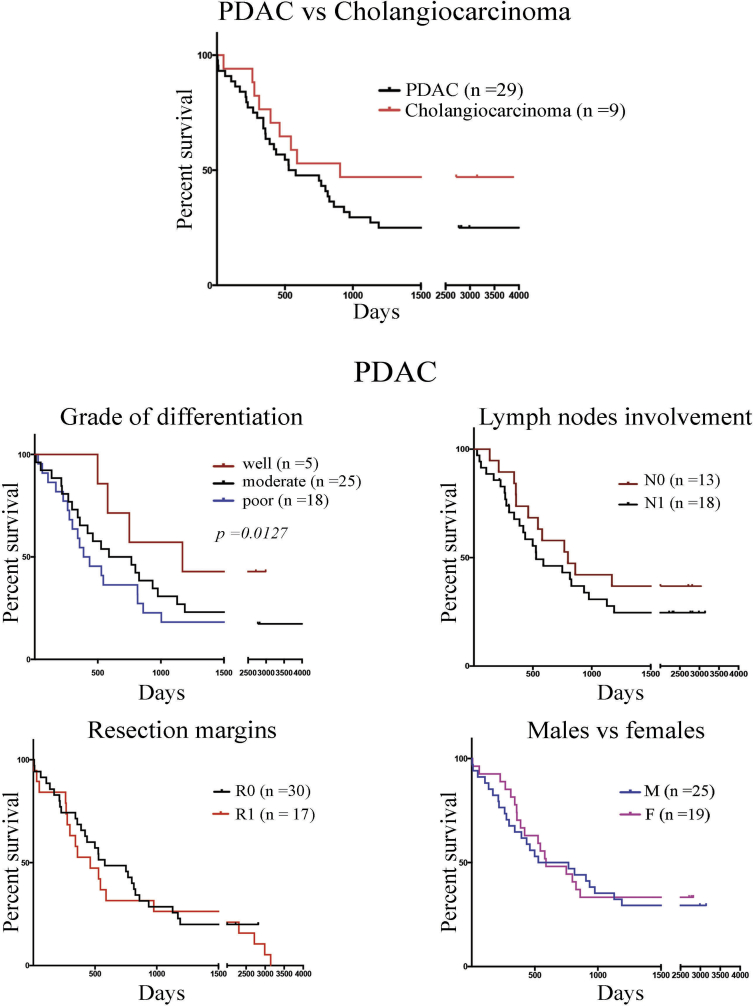
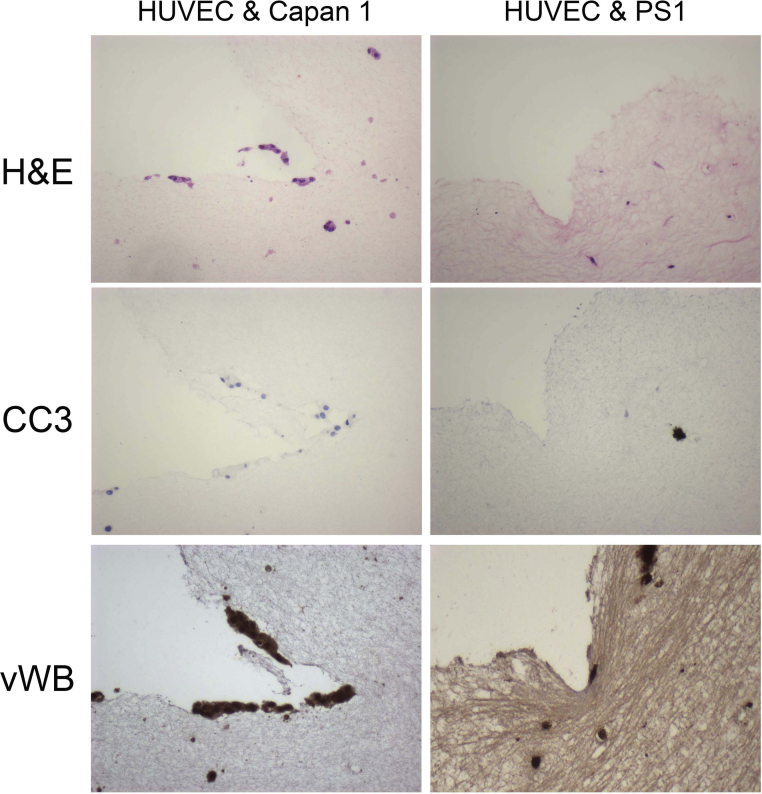
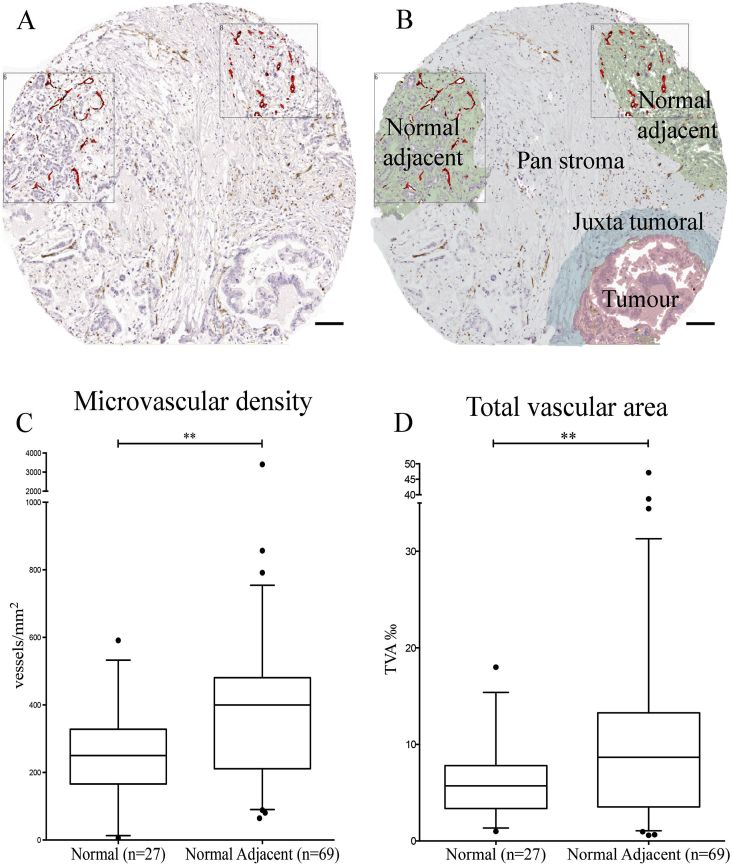
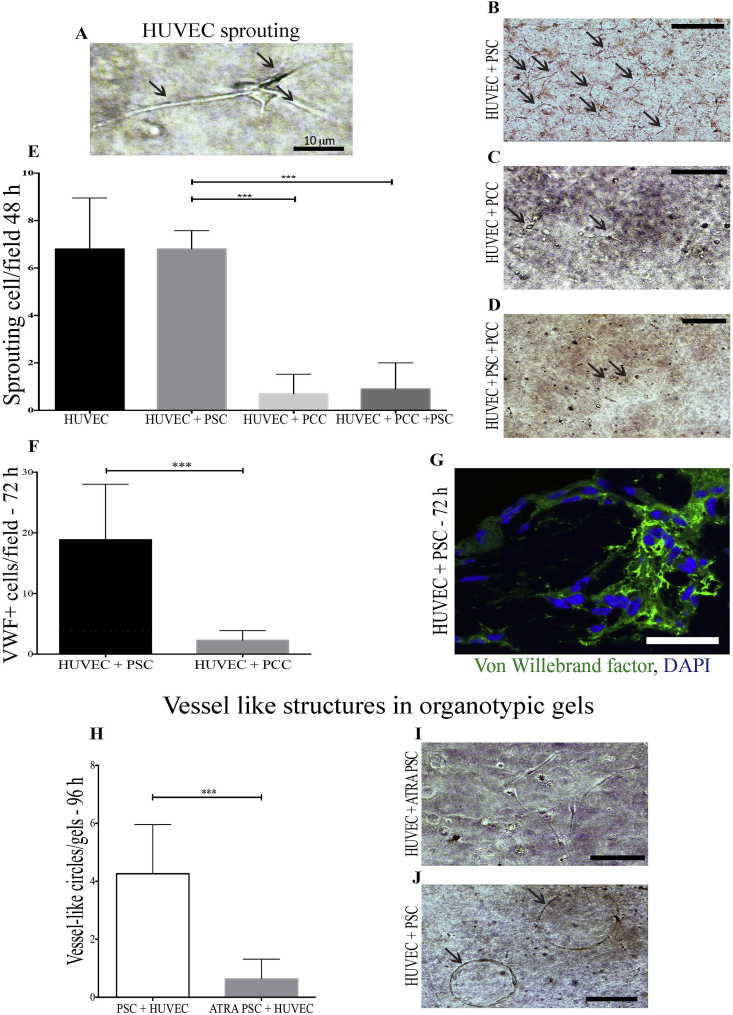
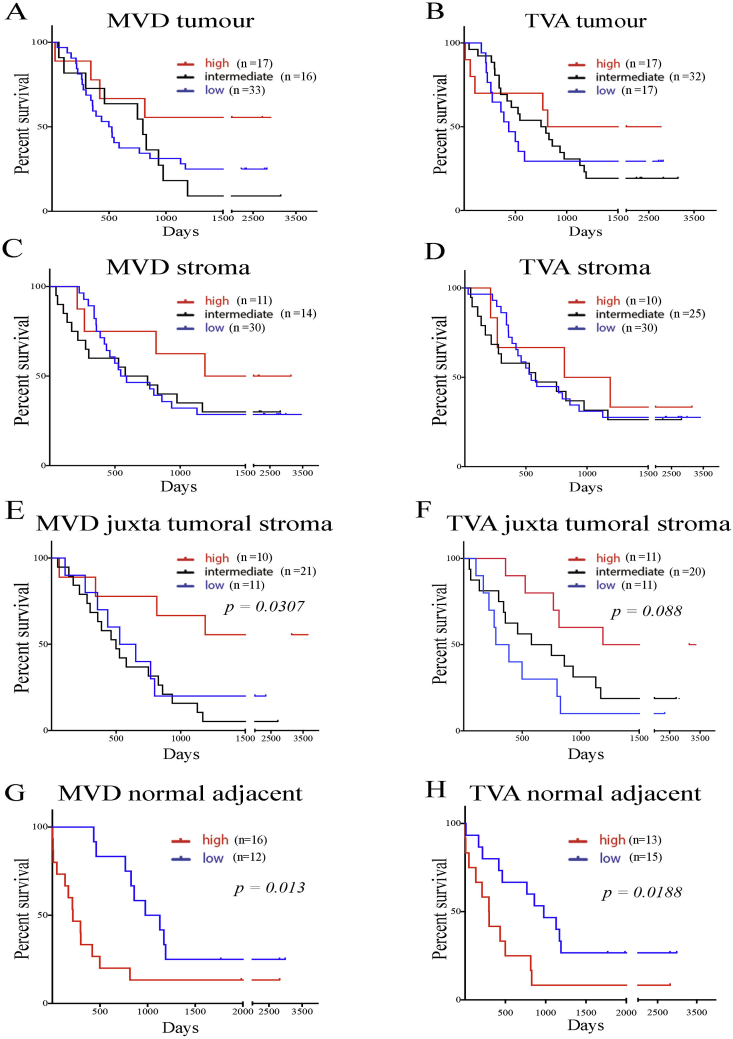
Results: PDAC has a distinct vascular density and distribution of vessels compared to cholangiocarcinoma. The PDAC juxta-tumoral stroma was hypovascular and the normal adjacent rim was hypervascular compared to the panstromal compartment. These features adversely affected patient prognosis, suggesting a model for spatio-temporal PDAC evolution. Mice aortic rings and 3D organotypic cultures demonstrated pro- and anti-angiogenic signalling from activated PSC and cancer cells respectively. ATRA-induced quiescence suppressed the pro-angiogenic activity of PSC.
Conclusion: Human PDAC has variable vascularity at microscopic level suggesting that novel stromal directed therapies would need to be determined by pathological characteristics.
Keywords: Angiogenesis; Juxta-tumoral; Micro-environment; Pancreatic stellate cells; Panstromal.
Copyright © 2016 IAP and EPC. Published by Elsevier B.V. All rights reserved.
Figures
References
-
- Wong P.P., Demircioglu F., Ghazaly E., Alrawashdeh W., Stratford M.R., Scudamore C.L. Dual-action combination therapy enhances angiogenesis while reducing tumor growth and spread. Cancer Cell. 2015;27(1):123–137. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
