

Systematic Molecular Phenotyping: A Path Toward Precision Emergency Medicine?
- PMID: 27288269
- PMCID: PMC5055430
- DOI: 10.1111/acem.13027
Systematic Molecular Phenotyping: A Path Toward Precision Emergency Medicine?
Abstract
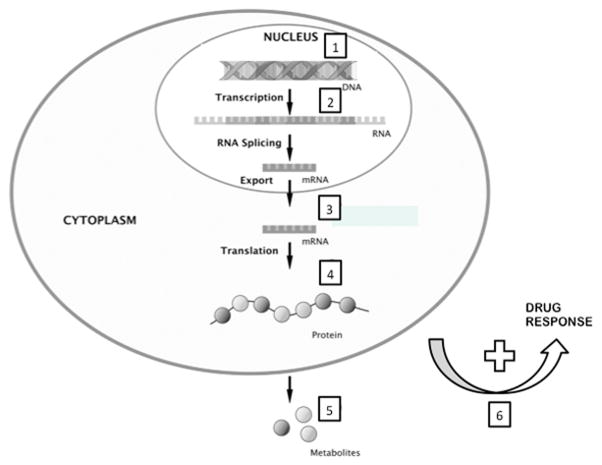
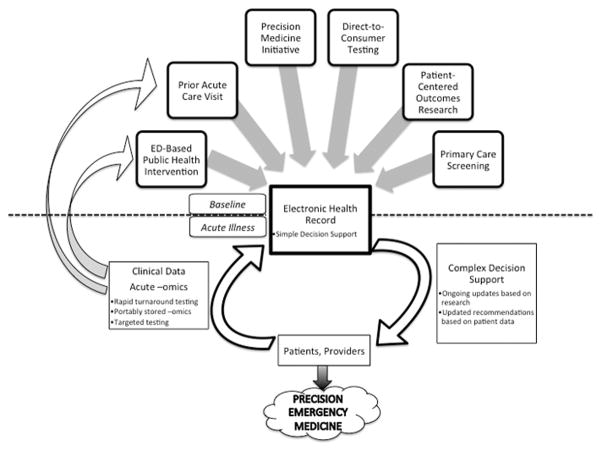
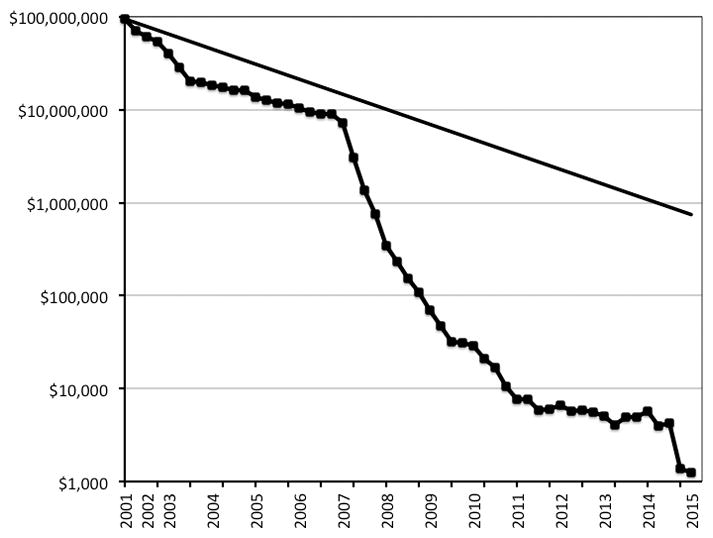
Precision medicine is an emerging approach to disease treatment and prevention that considers variability in patient genes, environment, and lifestyle. However, little has been written about how such research impacts emergency care. Recent advances in analytical techniques have made it possible to characterize patients in a more comprehensive and sophisticated fashion at the molecular level, promising highly individualized diagnosis and treatment. Among these techniques are various systematic molecular phenotyping analyses (e.g., genomics, transcriptomics, proteomics, and metabolomics). Although a number of emergency physicians use such techniques in their research, widespread discussion of these approaches has been lacking in the emergency care literature and many emergency physicians may be unfamiliar with them. In this article, we briefly review the underpinnings of such studies, note how they already impact acute care, discuss areas in which they might soon be applied, and identify challenges in translation to the emergency department (ED). While such techniques hold much promise, it is unclear whether the obstacles to translating their findings to the ED will be overcome in the near future. Such obstacles include validation, cost, turnaround time, user interface, decision support, standardization, and adoption by end-users.
© 2016 by the Society for Academic Emergency Medicine.
Conflict of interest statement
There are no relevant commercial conflicts of interest.
Figures
References
-
- [Accessed 6/2/15];International Consortium Completes Human Genome Project. 2003 at http://www.genome.gov/11006929. - PubMed
-
- Guinto J. Why is this $99 Home DNA Kit Causing Such an Uproar? Genome. 2014
-
- [Accessed 6/2/15];Optimizing FDA’s Regulatory Oversight of Next Generation Sequencing Diagnostic Tests—Preliminary Discussion Paper. 2015 at http://www.fda.gov/downloads/MedicalDevices/NewsEvents/WorkshopsConferen....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
