

Renal thrombotic microangiopathy in patients with cblC defect: review of an under-recognized entity
- PMID: 27289364
- PMCID: PMC5368212
- DOI: 10.1007/s00467-016-3399-0
Renal thrombotic microangiopathy in patients with cblC defect: review of an under-recognized entity
Abstract
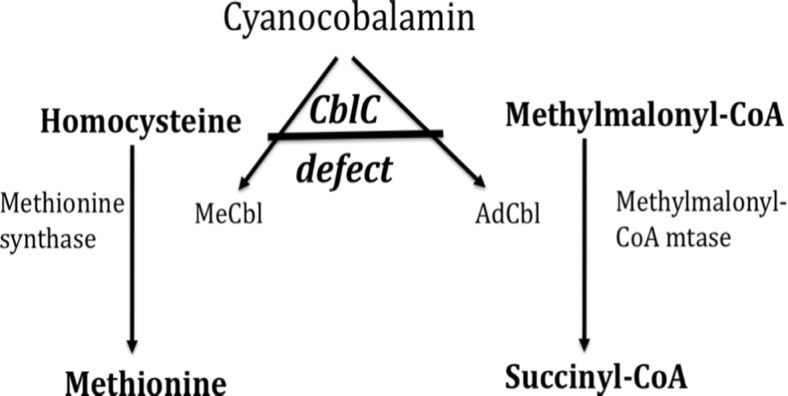
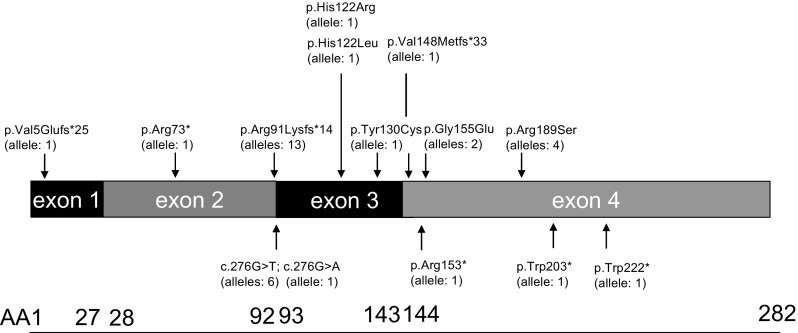
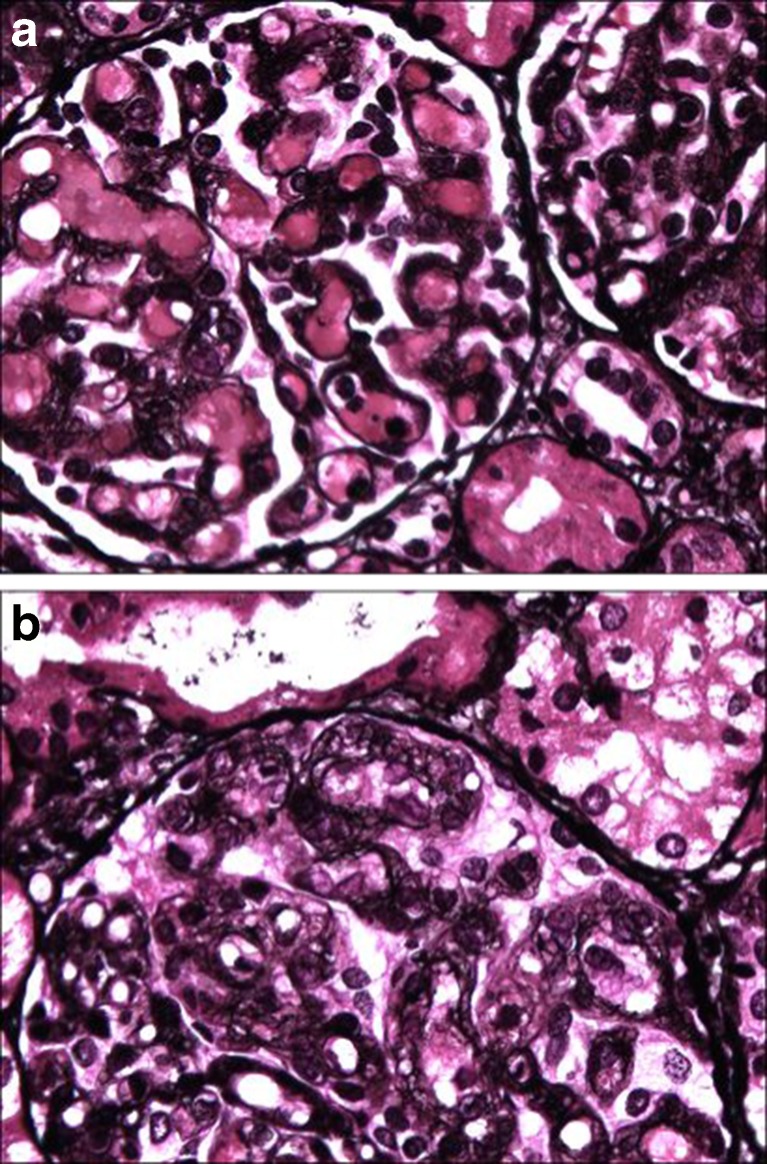
Methylmalonic aciduria and homocystinuria, cobalamin C (cblC) type, is the most common genetic type of functional cobalamin (vitamin B12) deficiency. This metabolic disease is characterized by marked heterogeneity of neurocognitive disease (microcephaly, seizures, developmental delay, ataxia, hypotonia) and variable extracentral nervous system involvement (failure to thrive, cardiovascular, renal, ocular) manifesting predominantly early in life, sometimes during gestation. To enhance awareness and understanding of renal disease associated with cblC defect, we studied biochemical, genetic, clinical, and histopathological data from 36 patients. Consistent clinical chemistry features of renal disease were intravascular hemolysis, hematuria, and proteinuria in all patients, with nephrotic-range proteinuria observed in three. Renal function ranged from normal to renal failure, with eight patients requiring (intermittent) dialysis. Two thirds were diagnosed with atypical (diarrhea-negative) hemolytic uremic syndrome (HUS). Renal histopathology analyses of biopsy samples from 16 patients revealed glomerular lesions typical of thrombotic microangiopathy (TMA). Treatment with hydroxycobalamin improved renal function in the majority, including three in whom dialysis could be withdrawn. Neurological sequelae were observed in 44 % and cardiopulmonary involvement in 39 % of patients, with half of the latter group demonstrating pulmonary hypertension. Mortality reached 100 % in untreated patients and 79 and 56 % in those with cardiopulmonary or neurological involvement, respectively. In all patients presenting with unclear intravascular hemolysis, hematuria, and proteinuria, cblC defect should be ruled out by determination of blood/plasma homocysteine levels and/or genetic testing, irrespective of actual renal function and neurological status, to ensure timely diagnosis and treatment.
Keywords: Atypical hemolytic uremic syndrome; Children; Cobalamin C defect; Pulmonary arterial hypertension.
Conflict of interest statement
The authors declare no conflict interest.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
