

Spatial niche formation but not malignant progression is a driving force for intratumoural heterogeneity
- PMID: 27291893
- PMCID: PMC4910022
- DOI: 10.1038/ncomms11845
Spatial niche formation but not malignant progression is a driving force for intratumoural heterogeneity
Abstract
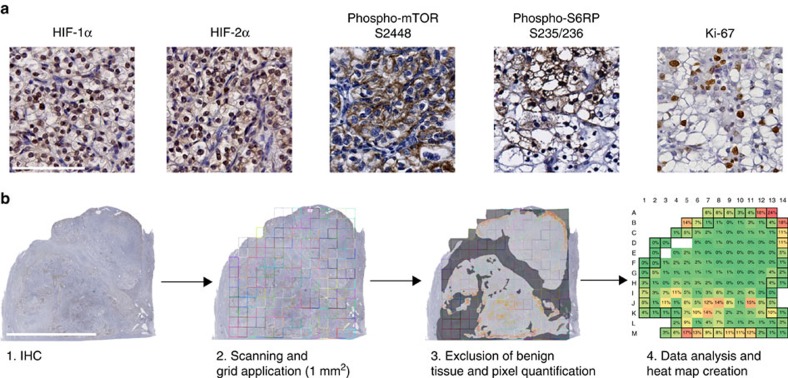
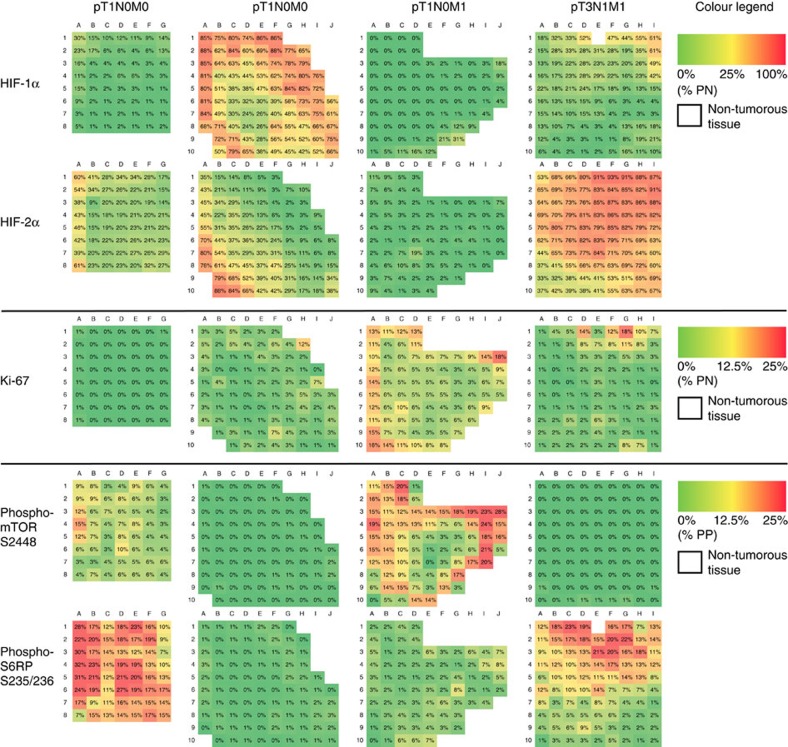
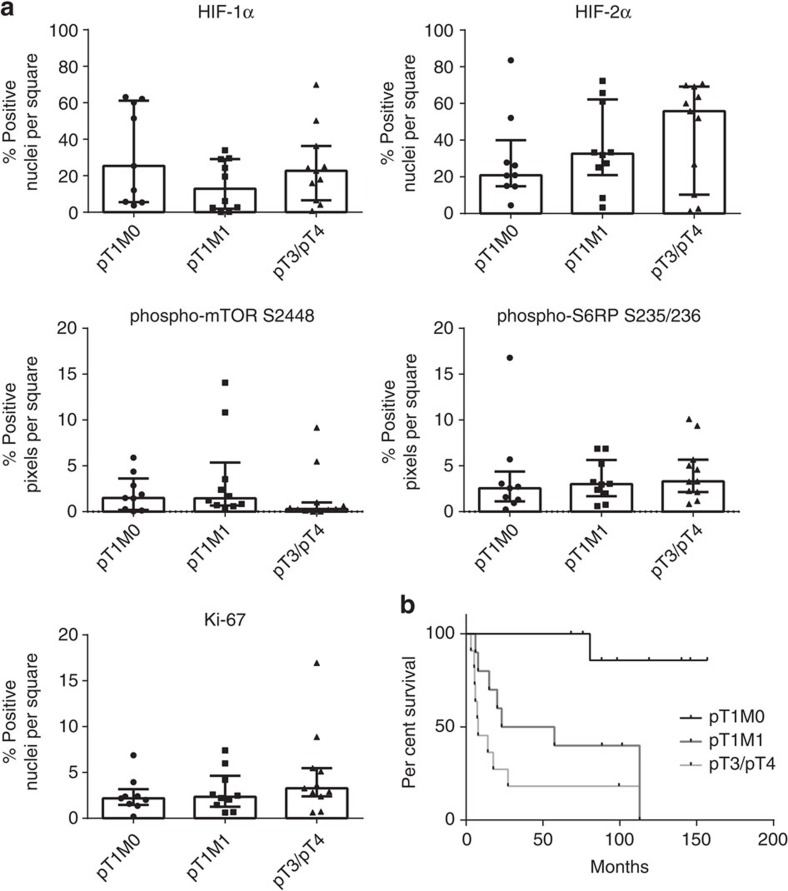
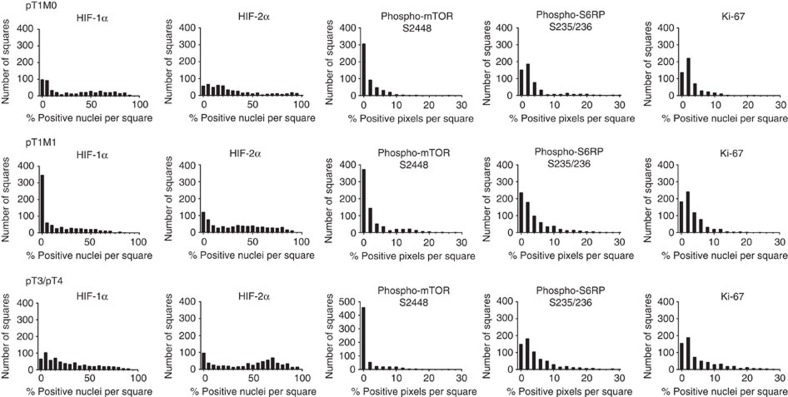
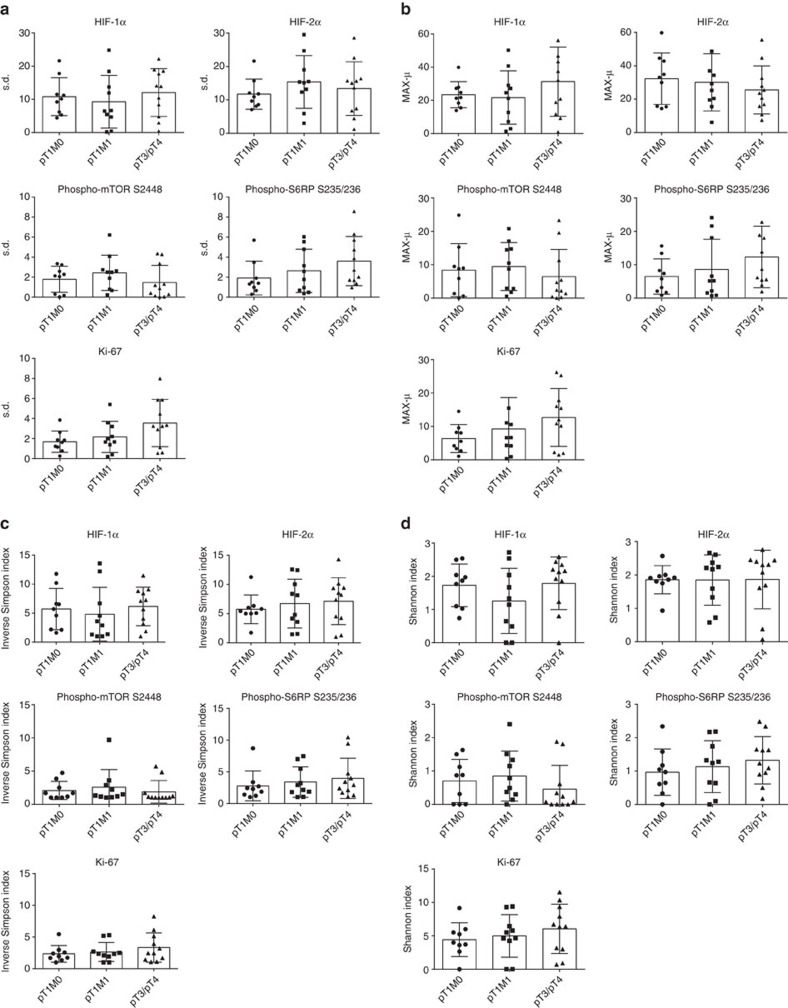
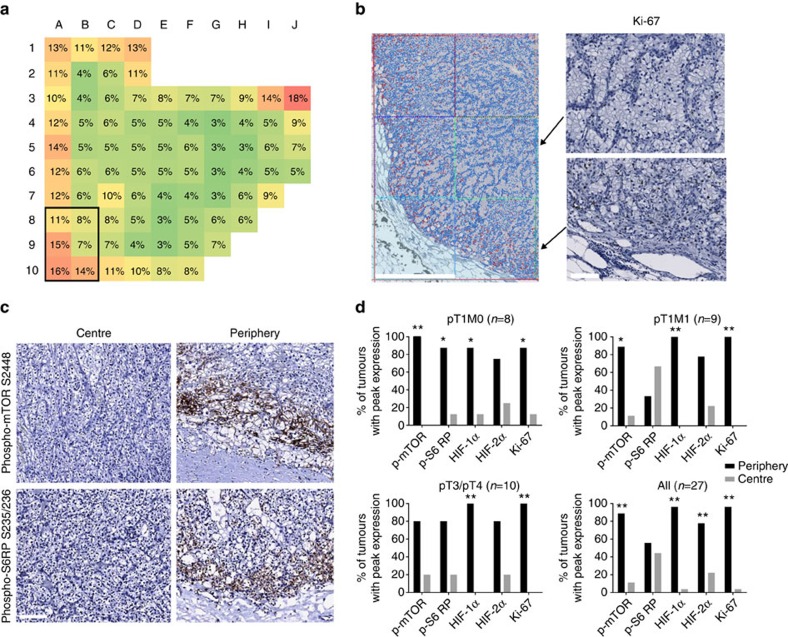
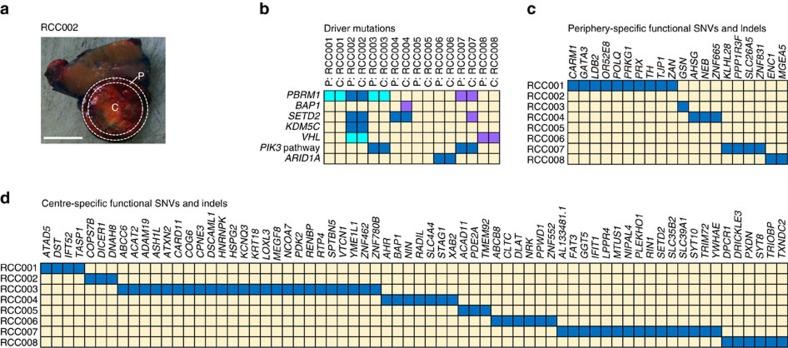
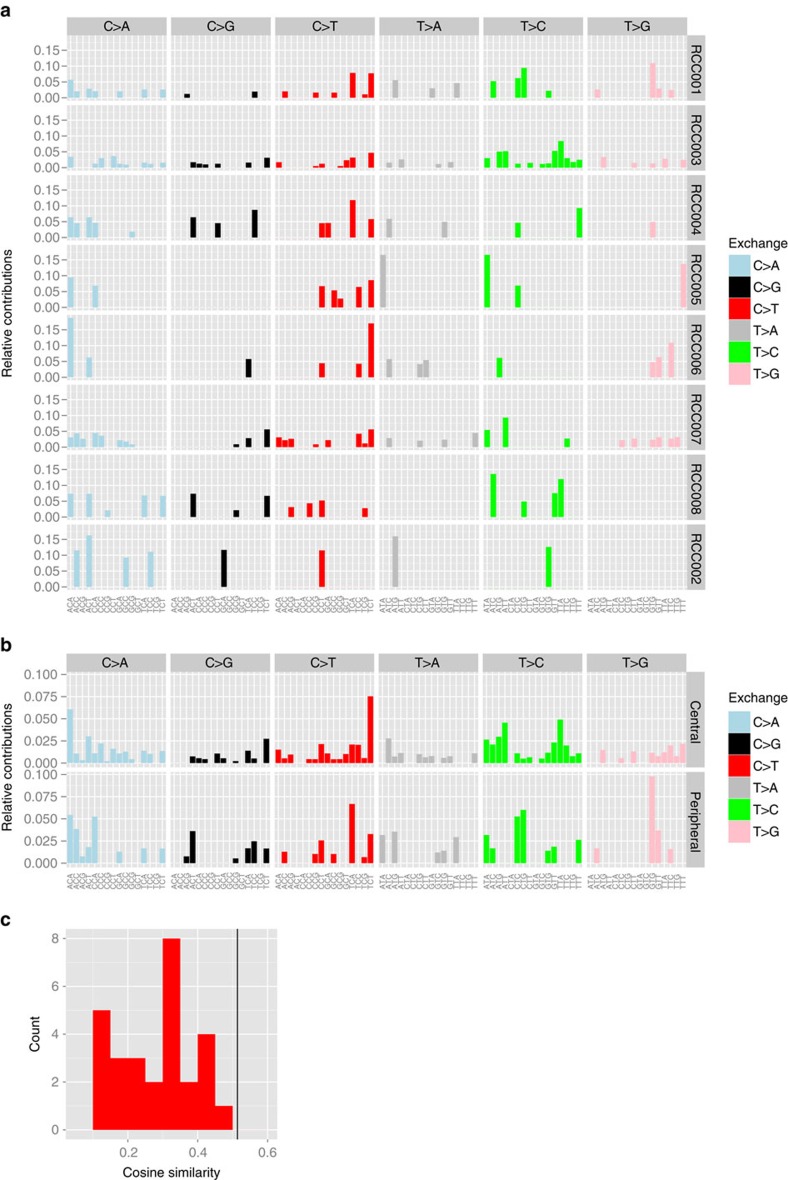
Intratumoural heterogeneity (ITH) is a major cause of cancer-associated lethality. Extensive genomic ITH has previously been reported in clear cell renal cell carcinoma (ccRCC). Here we address the question whether ITH increases with malignant progression and can hence be exploited as a prognostic marker. Unexpectedly, precision quantitative image analysis reveals that the degree of functional ITH is virtually identical between primary ccRCCs of the lowest stage and advanced, metastatic tumours. Functional ITH was found to show a stage-independent topological pattern with peak proliferative and signalling activities almost exclusively in the tumour periphery. Exome sequencing of matching peripheral and central primary tumour specimens reveals various region-specific mutations. However, these mutations cannot directly explain the zonal pattern suggesting a role of microenvironmental factors in shaping functional ITH. In conclusion, our results indicate that ITH is an early and general characteristic of malignant growth rather than a consequence of malignant progression.
Figures
References
-
- Nowell P. The clonal evolution of tumor cell populations. Science 194, 23–28 (1976). - PubMed
-
- Cahill D. P., Kinzler K. W., Vogelstein B. & Lengauer C. Genetic instability and darwinian selection in tumours. Trends Cell Biol. 9, M57–M60 (1999). - PubMed
-
- Burrell R. A., McGranahan N., Bartek J. & Swanton C. The causes and consequences of genetic heterogeneity in cancer evolution. Nature 501, 338–345 (2013). - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
