

Inotuzumab Ozogamicin versus Standard Therapy for Acute Lymphoblastic Leukemia
- PMID: 27292104
- PMCID: PMC5594743
- DOI: 10.1056/NEJMoa1509277
Inotuzumab Ozogamicin versus Standard Therapy for Acute Lymphoblastic Leukemia
Abstract
Background: The prognosis for adults with relapsed acute lymphoblastic leukemia is poor. We sought to determine whether inotuzumab ozogamicin, an anti-CD22 antibody conjugated to calicheamicin, results in better outcomes in patients with relapsed or refractory acute lymphoblastic leukemia than does standard therapy.
Methods: In this phase 3 trial, we randomly assigned adults with relapsed or refractory acute lymphoblastic leukemia to receive either inotuzumab ozogamicin (inotuzumab ozogamicin group) or standard intensive chemotherapy (standard-therapy group). The primary end points were complete remission (including complete remission with incomplete hematologic recovery) and overall survival.
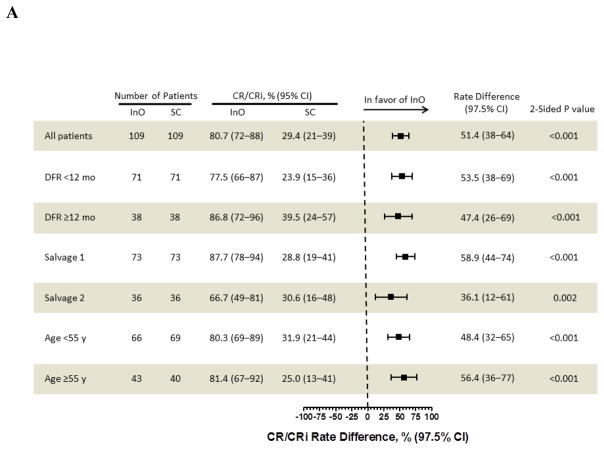
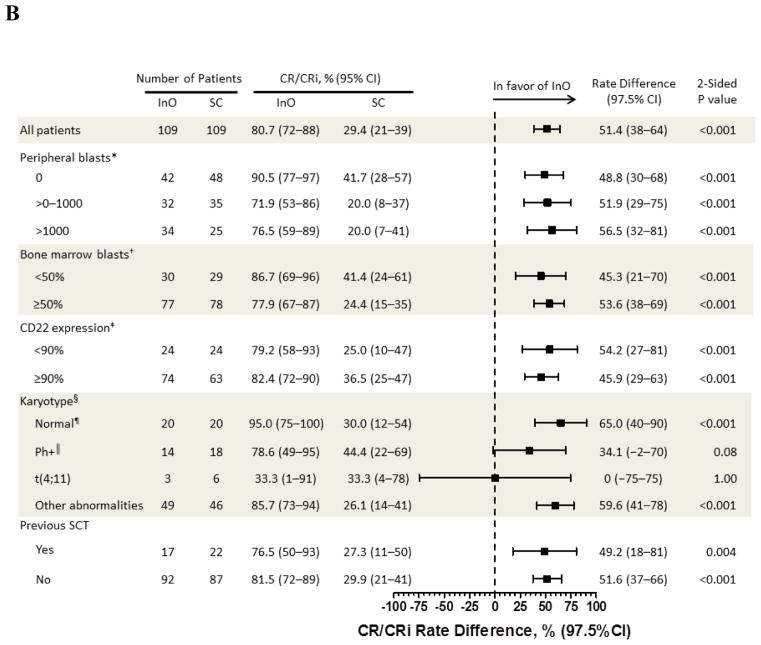
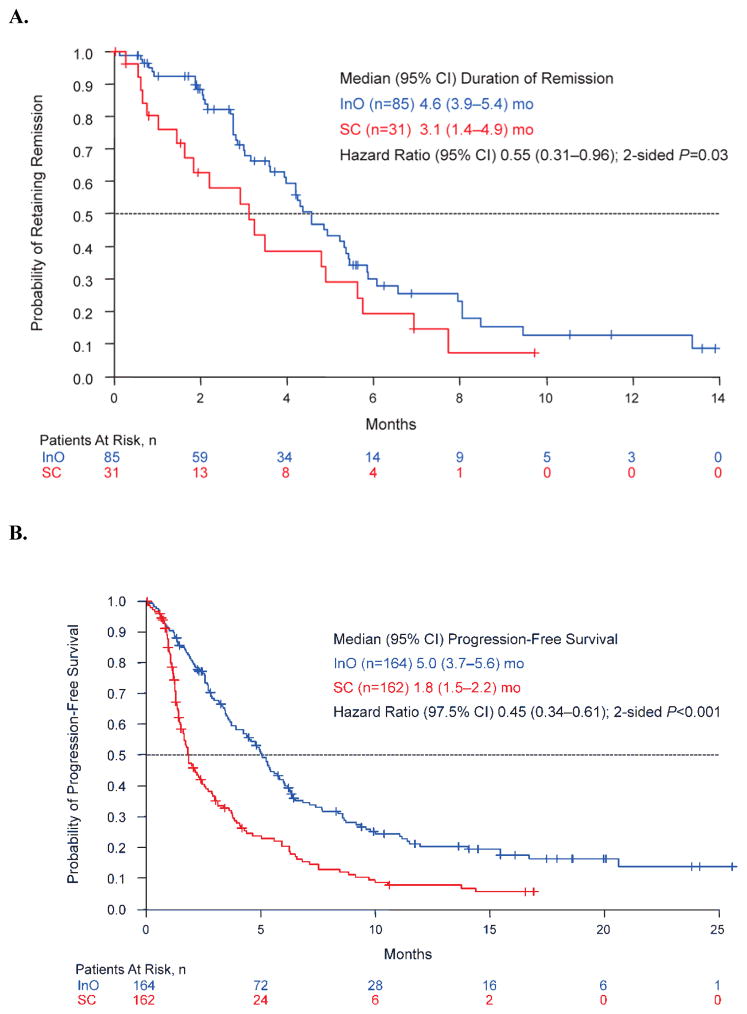
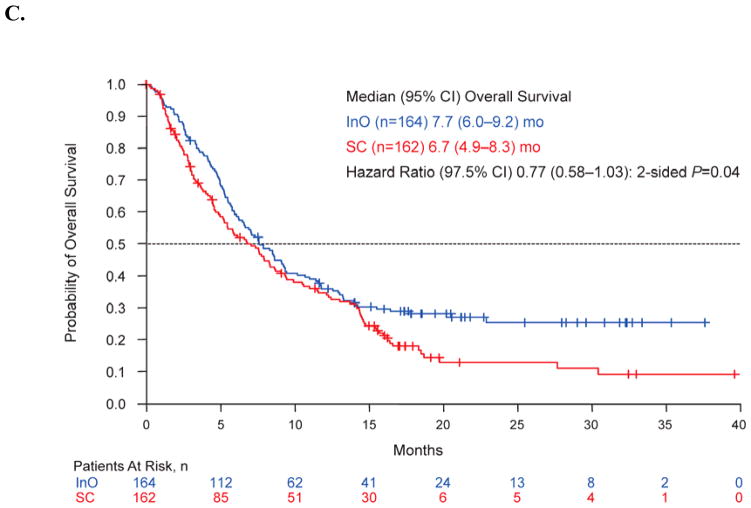
Results: Of the 326 patients who underwent randomization, the first 218 (109 in each group) were included in the primary intention-to-treat analysis of complete remission. The rate of complete remission was significantly higher in the inotuzumab ozogamicin group than in the standard-therapy group (80.7% [95% confidence interval {CI}, 72.1 to 87.7] vs. 29.4% [95% CI, 21.0 to 38.8], P<0.001). Among the patients who had complete remission, a higher percentage in the inotuzumab ozogamicin group had results below the threshold for minimal residual disease (0.01% marrow blasts) (78.4% vs. 28.1%, P<0.001); the duration of remission was longer in the inotuzumab ozogamicin group (median, 4.6 months [95% CI, 3.9 to 5.4] vs. 3.1 months [95% CI, 1.4 to 4.9]; hazard ratio, 0.55 [95% CI, 0.31 to 0.96]; P=0.03). In the survival analysis, which included all 326 patients, progression-free survival was significantly longer in the inotuzumab ozogamicin group (median, 5.0 months [95% CI, 3.7 to 5.6] vs. 1.8 months [95% CI, 1.5 to 2.2]; hazard ratio, 0.45 [97.5% CI, 0.34 to 0.61]; P<0.001); the median overall survival was 7.7 months (95% CI, 6.0 to 9.2) versus 6.7 months (95% CI, 4.9 to 8.3), and the hazard ratio was 0.77 (97.5% CI, 0.58 to 1.03) (P=0.04). In the safety population, the most frequent grade 3 or higher nonhematologic adverse events with inotuzumab ozogamicin were liver-related. Veno-occlusive liver disease of any grade occurred in 15 patients (11%) who received inotuzumab ozogamicin and in 1 patient (1%) who received standard therapy.
Conclusions: The rate of complete remission was higher with inotuzumab ozogamicin than with standard therapy, and a higher percentage of patients in the inotuzumab ozogamicin group had results below the threshold for minimal residual disease. Both progression-free and overall survival were longer with inotuzumab ozogamicin. Veno-occlusive liver disease was a major adverse event associated with inotuzumab ozogamicin. (Funded by Pfizer; INO-VATE ALL ClinicalTrials.gov number, NCT01564784.).
Figures
Comment in
-
Inotuzumab Ozogamicin for Acute Lymphoblastic Leukemia.N Engl J Med. 2016 Nov 24;375(21):2100-2101. doi: 10.1056/NEJMc1612040. N Engl J Med. 2016. PMID: 27959720 No abstract available.
-
Inotuzumab Ozogamicin for Acute Lymphoblastic Leukemia.N Engl J Med. 2016 Nov 24;375(21):2100. doi: 10.1056/NEJMc1612040. N Engl J Med. 2016. PMID: 27959721 No abstract available.
-
ADC Approval Likely to Spur More Research.Cancer Discov. 2017 Oct;7(10):1054-1055. doi: 10.1158/2159-8290.CD-NB2017-120. Epub 2017 Aug 29. Cancer Discov. 2017. PMID: 28851687
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. - PubMed
-
- Rowe JM, Buck G, Burnett AK, et al. Induction therapy for adults with acute lymphoblastic leukemia: results of more than 1500 patients from the international ALL trial: MRC UKALL XII/ECOG E2993. Blood. 2005;106:3760–7. - PubMed
-
- Goldstone AH, Richards SM, Lazarus HM, et al. In adults with standard-risk acute lymphoblastic leukemia, the greatest benefit is achieved from a matched sibling allogeneic transplantation in first complete remission, and an autologous transplantation is less effective than conventional consolidation/maintenance chemotherapy in all patients: final results of the International ALL Trial (MRC UKALL XII/ECOG E2993) Blood. 2008;111:1827–33. - PubMed
-
- Gokbuget N, Hoelzer D, Arnold R, et al. Treatment of Adult ALL according to protocols of the German Multicenter Study Group for Adult ALL (GMALL) Hematol Oncol Clin North Am. 2000;14:1307–25. ix. - PubMed
-
- Kantarjian H, Thomas D, O’Brien S, et al. Long-term follow-up results of hyperfractionated cyclophosphamide, vincristine, doxorubicin, and dexamethasone (Hyper-CVAD), a dose-intensive regimen, in adult acute lymphocytic leukemia. Cancer. 2004;101:2788–801. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical