

Management of post-operative pain by placement of an intraoperative intercostal catheter after single port video-assisted thoracoscopic surgery: a propensity-score matched study
- PMID: 27293824
- PMCID: PMC4885964
- DOI: 10.21037/jtd.2016.04.01
Management of post-operative pain by placement of an intraoperative intercostal catheter after single port video-assisted thoracoscopic surgery: a propensity-score matched study
Abstract
Background: The establishment of a golden standard for post-operative analgesia after thoracic surgery remains an unresolved issue. Benefiting from the rapid development of single port video-assisted thoracoscopic surgery (VATS), a good candidate for the alleviation of patients' pain is the placement of an intercostal catheter (ICC) safely after uniport VATS. We hypothesized that continual infusion through ICC could provide effective analgesia for patients with only one wound and we evaluate its postoperative analgesic function in uniport VATS patients with or without intercostal nerve blockade.
Methods: Since March 2014, 235 patients received various kinds of single port VATS. We identified 50 patients who received single port VATS with intercostal nerve blockade and retrospectively compared them with a group of patients who had received single port VATS without intercostal nerve blockade. The operative time, post operation day 0, 1, 2, 3 and discharge day pain score, narcotic requirements, drainage duration and post-operative hospital stay were collected. In order to establish a well-balanced cohort study, we also used propensity scores matching (1:1) to compare the short term clinical outcome in two groups.
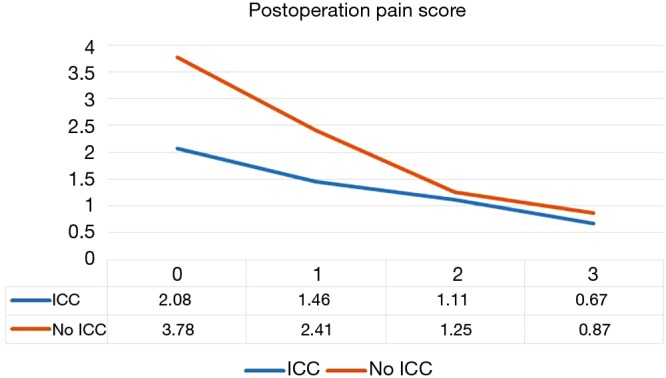
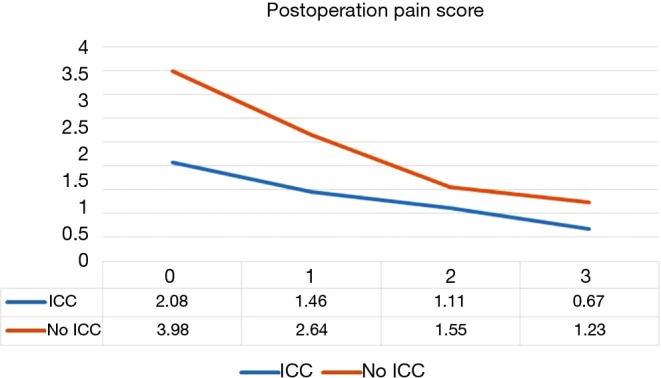
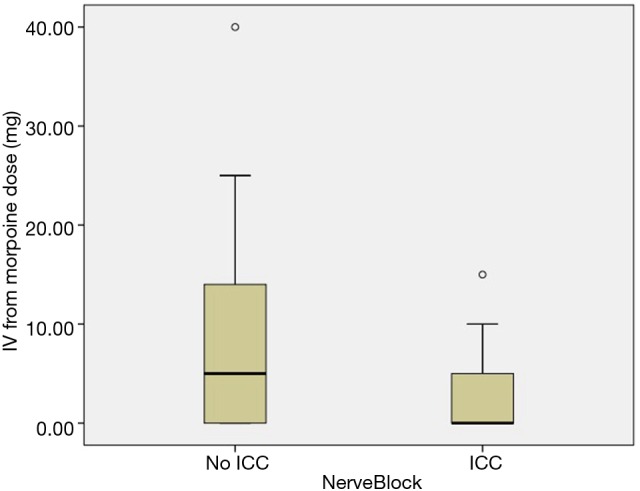
Results: No operative deaths occurred in this study. The uniport VATS with intercostal nerve blockade group was associated with less post operation day 0 and day 1 pain score, and narcotic requirements in our cohort study (P<0.001, <0.001, and 0.003). After propensity scores matching, there were 50 patients in each group. Mean day 0 and day 1, day 2, day 3 pain score, drainage duration, post-operative hospital stay, and narcotic requirements were smaller in uniport VATS with intercostal nerve blockade (P<0.001, <0.001, 0.038, 0.007, 0.02, 0.042, and 0.003).
Conclusions: In conclusion, in patients post single port VATS, continual intercostal nerve block with levobupivacaine infusion appears to be a safe, effective and promising technique in our study, associated with a shorter hospital stay and less post-operative pain. Further prospective trials are needed to determine the long term outcomes.
Keywords: Minimally invasive surgery; intercostal nerve block; single port video-assisted thoracoscopic surgery (VATS).
Conflict of interest statement
Figures
Similar articles
-
Management of acute postoperative pain with continuous intercostal nerve block after single port video-assisted thoracoscopic anatomic resection.J Thorac Dis. 2016 Dec;8(12):3563-3571. doi: 10.21037/jtd.2016.12.30. J Thorac Dis. 2016. PMID: 28149550 Free PMC article.
-
Postoperative pain control with continuous paravertebral nerve block and intercostal nerve block after two-port video-assisted thoracic surgery.Wideochir Inne Tech Maloinwazyjne. 2021 Mar;16(1):273-281. doi: 10.5114/wiitm.2020.99349. Epub 2020 Sep 25. Wideochir Inne Tech Maloinwazyjne. 2021. PMID: 33786144 Free PMC article.
-
The perioperative outcomes of uniport versus two-port and three-port video-assisted thoracoscopic surgery in lung cancer: a systematic review and meta-analysis.J Cardiothorac Surg. 2022 Nov 8;17(1):284. doi: 10.1186/s13019-022-02034-y. J Cardiothorac Surg. 2022. PMID: 36348498 Free PMC article.
-
Comparative Short-Term Clinical Outcomes of Mediastinum Tumor Excision Performed by Conventional VATS and Single-Port VATS: Is It Worthwhile?Medicine (Baltimore). 2015 Nov;94(45):e1975. doi: 10.1097/MD.0000000000001975. Medicine (Baltimore). 2015. PMID: 26559275 Free PMC article.
-
Is uniport thoracoscopic surgery less painful than multiple port approaches?Interact Cardiovasc Thorac Surg. 2015 Mar;20(3):409-14. doi: 10.1093/icvts/ivu391. Epub 2014 Dec 3. Interact Cardiovasc Thorac Surg. 2015. PMID: 25472978 Review.
Cited by
-
Assessment of Intercostal Nerve Block Analgesia for Thoracic Surgery: A Systematic Review and Meta-analysis.JAMA Netw Open. 2021 Nov 1;4(11):e2133394. doi: 10.1001/jamanetworkopen.2021.33394. JAMA Netw Open. 2021. PMID: 34779845 Free PMC article.
-
Peripheral regional anaesthesia and outcomes: a narrative review of the literature from 2013 to 2023.Br J Anaesth. 2024 May;132(5):1082-1096. doi: 10.1016/j.bja.2023.10.013. Epub 2023 Nov 11. Br J Anaesth. 2024. PMID: 37957079 Free PMC article. Review.
-
Analgesic management after thoracoscopic surgery: recent studies and our experience.J Thorac Dis. 2018 Apr;10(Suppl 9):S1050-S1054. doi: 10.21037/jtd.2018.04.34. J Thorac Dis. 2018. PMID: 29849207 Free PMC article. No abstract available.
-
Is intensive care necessary after major thoracic surgery? A propensity score-matched study.Turk Gogus Kalp Damar Cerrahisi Derg. 2023 Apr 28;31(2):229-238. doi: 10.5606/tgkdc.dergisi.2023.23501. eCollection 2023 Apr. Turk Gogus Kalp Damar Cerrahisi Derg. 2023. PMID: 37484638 Free PMC article.
-
What is the best pain control after thoracic surgery?J Thorac Dis. 2018 Mar;10(3):1335-1338. doi: 10.21037/jtd.2018.03.63. J Thorac Dis. 2018. PMID: 29708130 Free PMC article. No abstract available.
References
-
- van Kleef JW, Logeman EA, Burm AG, et al. Continuous interpleural infusion of bupivacaine for postoperative analgesia after surgery with flank incisions: a double-blind comparison of 0.25% and 0.5% solutions. Anesth Analg 1992;75:268-74. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical