

For non-small cell lung cancer with T3 (central) disease, sleeve lobectomy or pneumonectomy?
- PMID: 27293841
- PMCID: PMC4886029
- DOI: 10.21037/jtd.2016.04.60
For non-small cell lung cancer with T3 (central) disease, sleeve lobectomy or pneumonectomy?
Abstract
Background: Pneumonectomy (PN) has traditionally been the treatment of choice for central lung tumors for which the alternative is sleeve lobectomy (SL). The aim of this study was to compare early and long-term results after SL and PN in focusing on T3 central non-small cell lung cancer (NSCLC).
Methods: Patients who underwent SL (n=58) or PN (n=42) were retrospectively analyzed. For bias reduction, these 100 patients had been selected according to the following criteria: (I) tumor located in the main bronchus less than 2 cm distal to the carina; (II) there were no N2 disease; (III) no induction therapy was applied; (IV) complete resection (R0) was achieved.
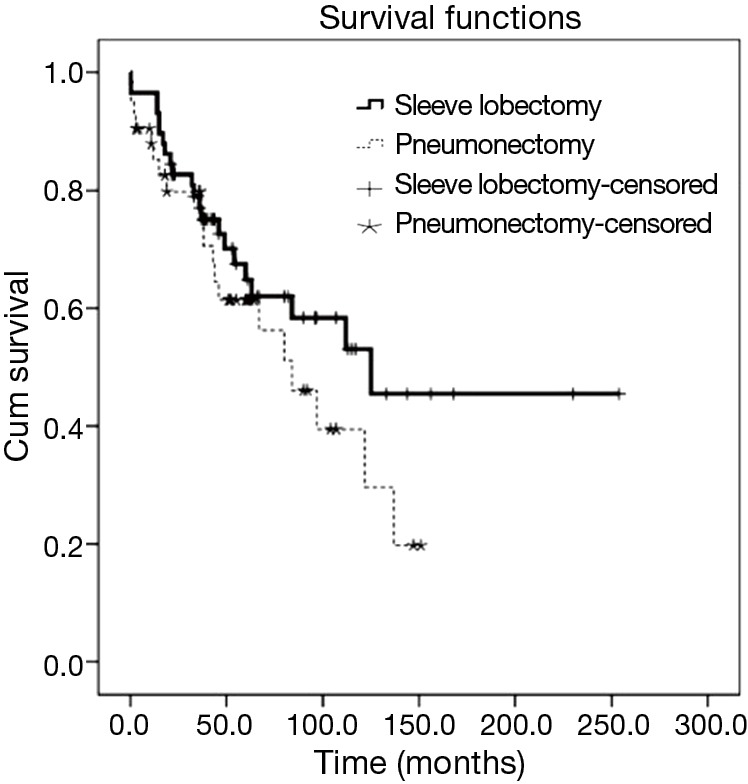
Results: SL and PN patients had comparable mean ages, gender distribution, mean forced expiratory volume in 1 second (FEV1), stage and tumor grade. Postoperative mortality (3.4% vs. 4.8%, P=1.0) and morbidity (41% vs. 38%, P=0.74) were similar between the two groups. Recurrences occurred in 48% of patients after SL and in 31% of those after PN (P=0.08). The 5-year survival after SL (64.8%) and PN (61.4%) was not significantly different (P=0.20). Multivariable survival analysis showed that there were no independent prognostic factors.
Conclusions: SL does not compromise survival for NSCLC with T3 central disease compared with PN. It is an adequate oncologic resection and should be treated as the first line intervention whenever complete resection can be achieved.
Keywords: Sleeve lobectomy (SL); lung neoplasm; pneumonectomy (PN).
Conflict of interest statement
Figures
References
-
- Wain JC. Bronchoplastic Resections. In: Kaiser LR. editor. Mastery of Cardiothoracic Surgery. Philadelphia: Lippincott-Raven, 1998:68-76.
-
- Ma Z, Dong A, Fan J, et al. Does sleeve lobectomy concomitant with or without pulmonary artery reconstruction (double sleeve) have favorable results for non-small cell lung cancer compared with pneumonectomy? A meta-analysis. Eur J Cardiothorac Surg 2007;32:20-8. 10.1016/j.ejcts.2007.03.018 - DOI - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources