

Lung B-line artefacts and their use
- PMID: 27293860
- PMCID: PMC4885976
- DOI: 10.21037/jtd.2016.04.55
Lung B-line artefacts and their use
Abstract
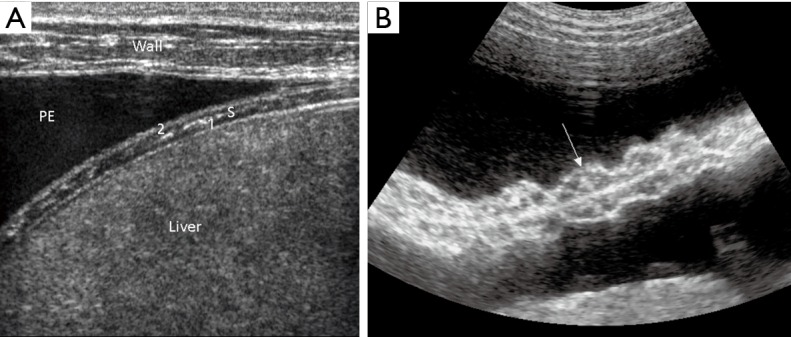
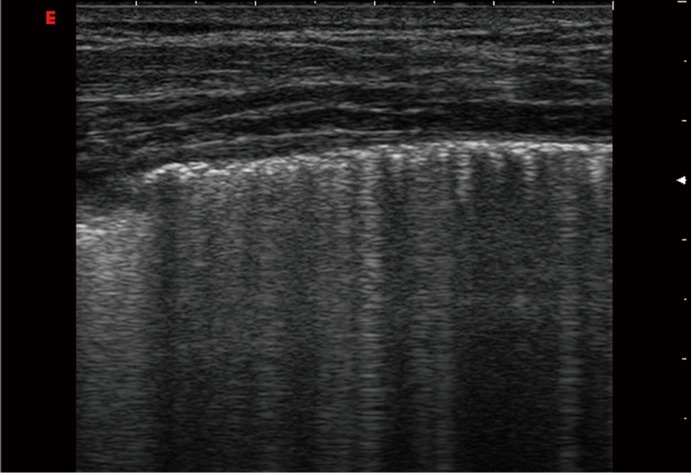
Background: The analysis of lung artefacts has gained increasing importance as markers of lung pathology. B-line artefact (BLA), caused by a reverberation phenomenon, is the most important lung artefact. In this review, we discuss the current role of BLA in pneumology and explore open questions of the published consensus.
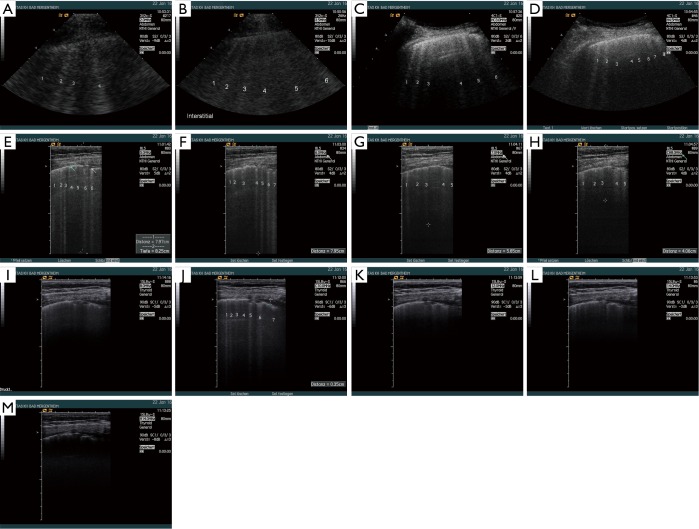
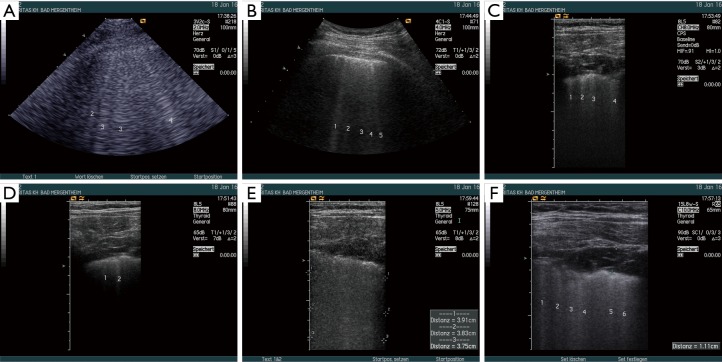
Methods: We summarized current literature about BLA. Also, we presented observations on healthy subjects and patients with interstitial syndrome (pulmonary fibrosis and edema), to investigate technical factors influencing BLA visualization.
Results: BLA imaging is influenced by more factors than recently assumed. When multiple BLA is visualized in the lung, they represent a sign of increased density due to the loss of aeration in the lung periphery. This condition may indicate different diseases including cardiogenic pulmonary edema, diffuse or focal interstitial lung diseases (ILD), infections and acute respiratory distress syndrome (ARDS). Correct interpretation of BLA in lung ultrasound is strongly influenced by associated sonographic signs and careful integration of all relevant clinical information.
Conclusions: BLA is useful to monitor clinical response, and may become crucial in directing the diagnostic process. Further research is warranted to clarify technical adjustments, different probe and machine factors that influence the visualization of BLA.
Keywords: Guidelines; atelectasis; consolidations; interstitial syndrome; malignancies; pleural effusion (PE); pneumonia; pulmonary thromboembolism.
Conflict of interest statement
Figures


References
-
- Volpicelli G. Lung sonography. J Ultrasound Med 2013;32:165-71. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources