

Is the intraoperative air leak test effective in the prevention of colorectal anastomotic leakage? A systematic review and meta-analysis
- PMID: 27294661
- PMCID: PMC4947486
- DOI: 10.1007/s00384-016-2616-4
Is the intraoperative air leak test effective in the prevention of colorectal anastomotic leakage? A systematic review and meta-analysis
Abstract
Objective: The intra-operative air leak test (ALT) is a common intraoperative test used to identify mechanically insufficient anastomosis. This meta-analysis aims to determine whether ALT aids to the reduction of postoperative colorectal anastomotic leakage (CAL).
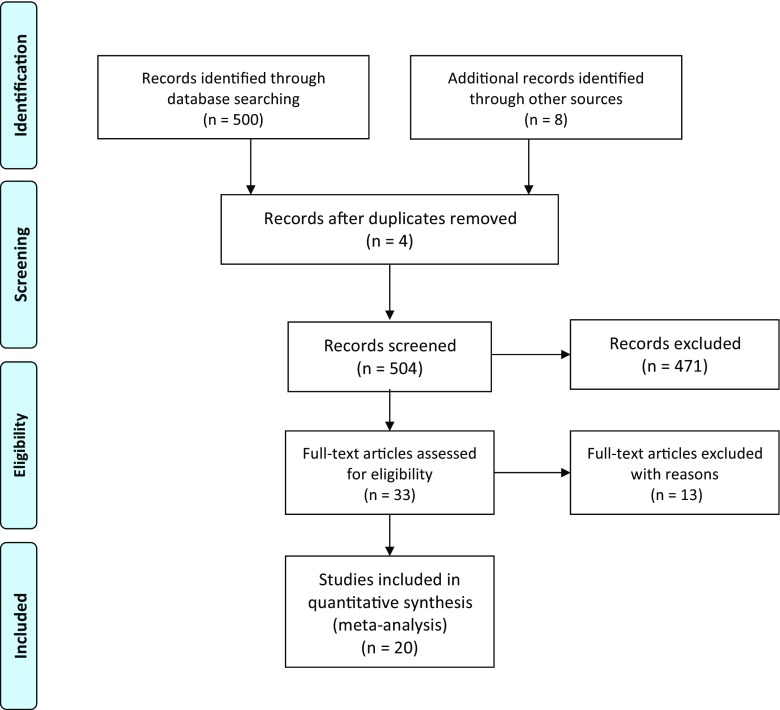
Methods: A literature search was performed to select studies in acknowledged databases. Full text articles targeting ALT during colorectal surgery were included. Quality assessment, risk of bias, and the level-of-evidence of the inclusions were evaluated. ALT methodology, ALT(+) (i.e., leak observed during the test) rate, and postoperative CAL rate of the included studies were subsequently analyzed.
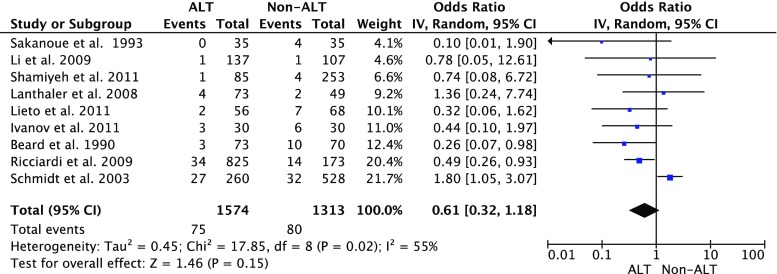
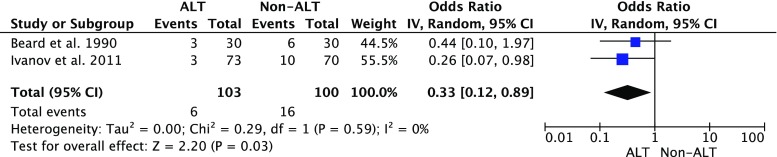
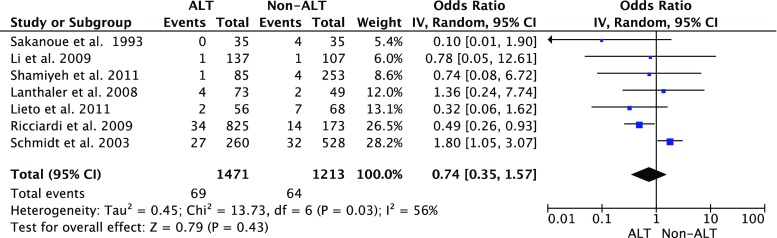
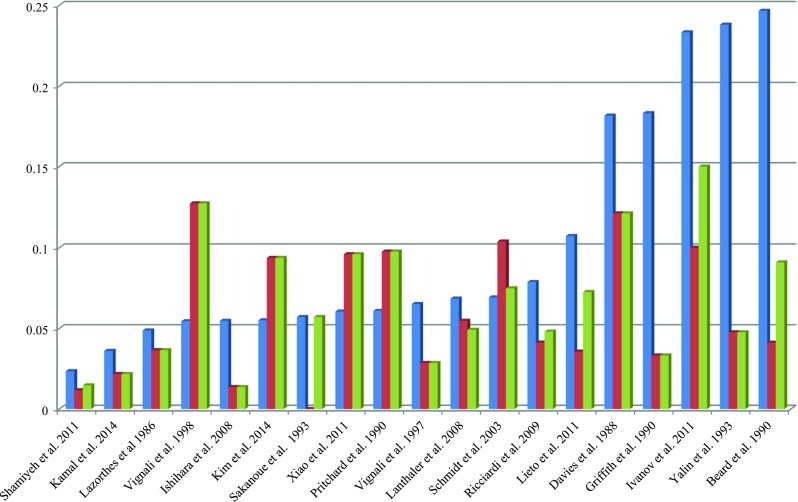
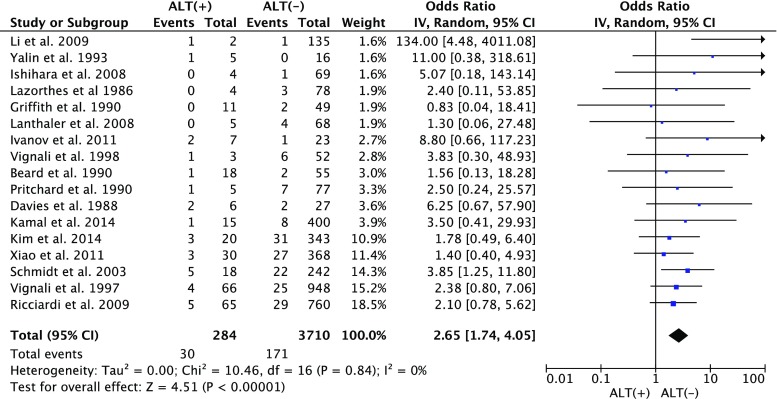
Results: Twenty studies were included for analysis, in which we found substantial risks of bias. A lower CAL rate was observed in patients who underwent ALT than those did not; however, the difference was not significant (p = 0.15). The intraoperative ALT(+) rate greatly varied among the included studies from 1.5 to 24.7 %. ALT(+) patients possessed a significantly higher CAL rate than the ALT(-) patients (11.4 vs. 4.2 %, p < 0.001).
Conclusions: Based on the available evidence, performing an ALT with the reported methodology has not significantly reduced the clinical CAL rate but remains necessary due to a higher risk of CAL in ALT(+) cases. Unfortunately, additional repairs under current methods may not effectively decrease this risk. Results of this review urge a standardization of ALT methodology and effective methods to repair ALT(+) anastomoses.
Keywords: Air leak test; Anastomotic leakage; Colorectal surgery; Prevention.
Figures
References
-
- Geoge WD (1991) Suturing or stapling in gastrointestinal surgery: a prospective randomized study. West of Scotland and Highland anastomosis study group. Br J Surg 78(3):337–341 - PubMed
-
- Group OLoEW (2011) The Oxford 2011 levels of evidence. Oxford centre for evidence-based medicine
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
