

A Multifactorial Weight Reduction Programme for Children with Overweight and Asthma: A Randomized Controlled Trial
- PMID: 27294869
- PMCID: PMC4905647
- DOI: 10.1371/journal.pone.0157158
A Multifactorial Weight Reduction Programme for Children with Overweight and Asthma: A Randomized Controlled Trial
Erratum in
-
Correction: A Multifactorial Weight Reduction Programme for Children with Overweight and Asthma: A Randomized Controlled Trial.PLoS One. 2017 Jul 6;12(7):e0181130. doi: 10.1371/journal.pone.0181130. eCollection 2017. PLoS One. 2017. PMID: 28683100 Free PMC article.
Abstract
Background: There is increasing evidence that obesity is related to asthma development and severity. However, it is largely unknown whether weight reduction can influence asthma management, especially in children.
Objective: To determine the effects of a multifactorial weight reduction intervention on asthma management in overweight/obese children with (a high risk of developing) asthma.
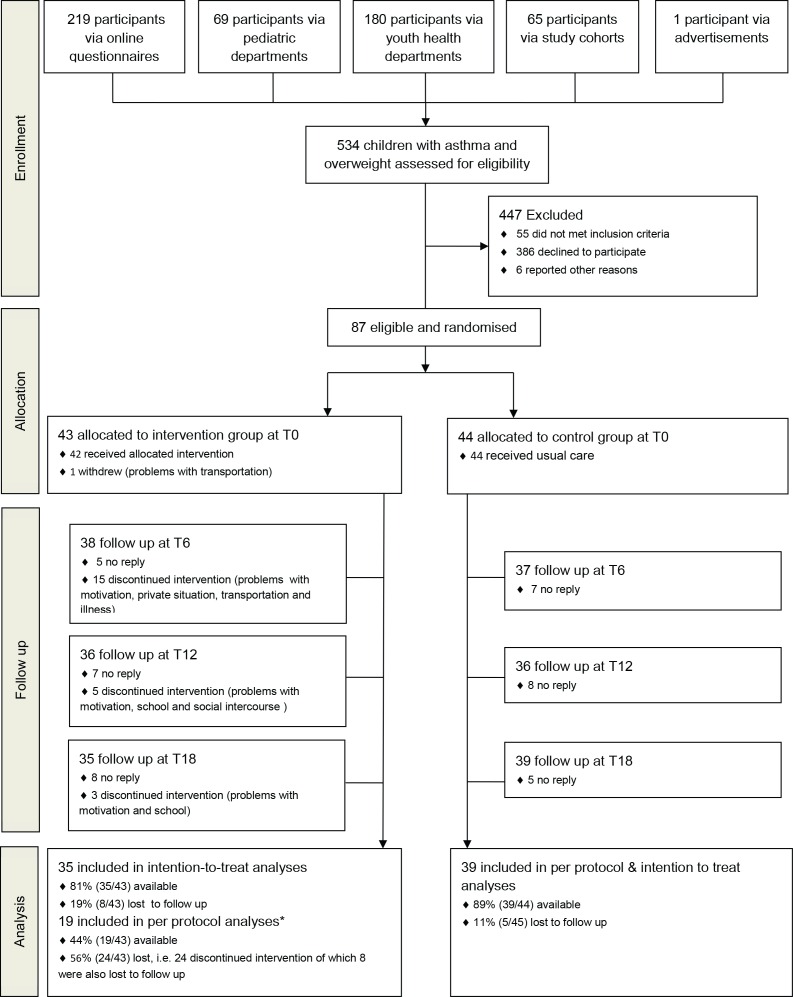
Methods: An 18-month weight-reduction randomized controlled trial was conducted in 87 children with overweight/obesity and asthma. Every six months, measurements of anthropometry, lung function, lifestyle parameters and inflammatory markers were assessed. Analyses were performed with linear mixed models for longitudinal analyses.
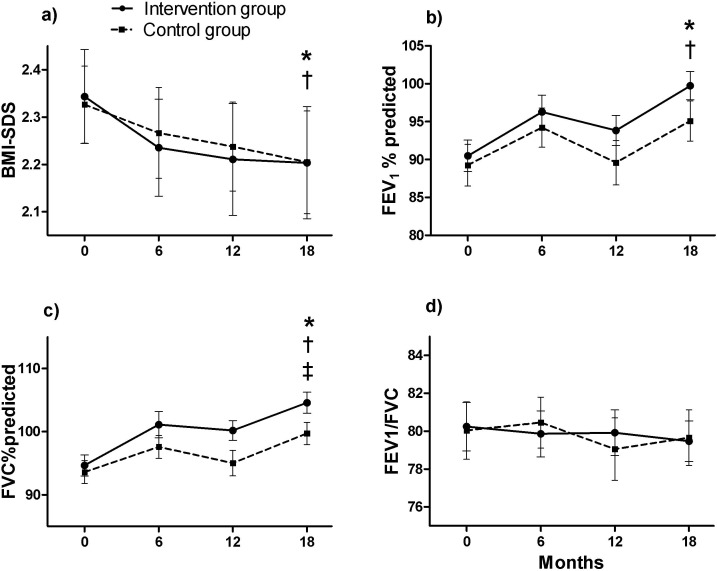
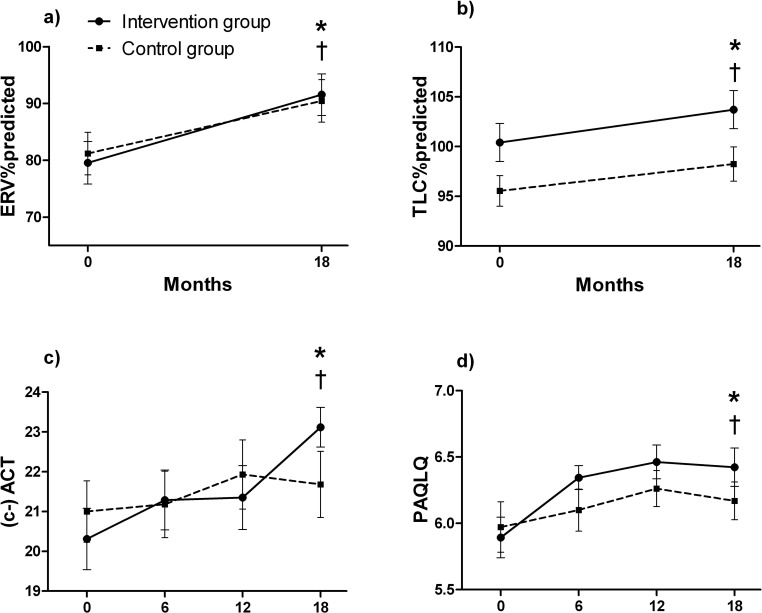
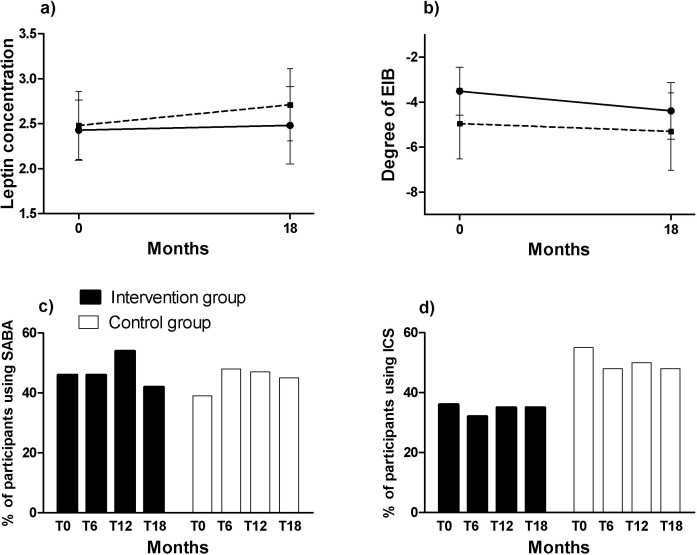
Results: After 18 months, the body mass index-standard deviation score decreased by -0.14±0.29 points (p<0.01) in the intervention group and -0.12±0.34 points (p<0.01) in the control group. This change over time did not differ between groups (p>0.05). Asthma features (including asthma control and asthma-related quality of life) and lung function indices (static and dynamic) improved significantly over time in both groups. The FVC% predicted improved over time by 10.1 ± 8.7% in the intervention group (p<0.001), which was significantly greater than the 6.1 ± 8.4% in the control group (p<0.05).
Conclusions & clinical relevance: Clinically relevant improvements in body weight, lung function and asthma features were found in both the intervention and control group, although some effects were more pronounced in the intervention group (FVC, asthma control, and quality of life). This implies that a weight reduction intervention could be clinically beneficial for children with asthma.
Trial registration: ClinicalTrials.gov NCT00998413.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
