

Aspergillus-positive lower respiratory tract samples in patients with the acute respiratory distress syndrome: a 10-year retrospective study
- PMID: 27294891
- PMCID: PMC4906097
- DOI: 10.1186/s13613-016-0156-2
Aspergillus-positive lower respiratory tract samples in patients with the acute respiratory distress syndrome: a 10-year retrospective study
Abstract
Background: The detection of Aspergillus spp. in endotracheal aspirate cultures of mechanically ventilated patients may reflect either colonization or infection. However, little is known about the prevalence and the impact on outcome of respiratory tract sample positive for Aspergillus during the acute respiratory distress syndrome (ARDS).
Methods: We conducted a monocentric, retrospective study over a 10-year period (January 2006-December 2015) in the ICU of a university hospital. All consecutive adult patients with ARDS were included, and the diagnosis of invasive pulmonary aspergillosis was assessed using a previously validated algorithm.
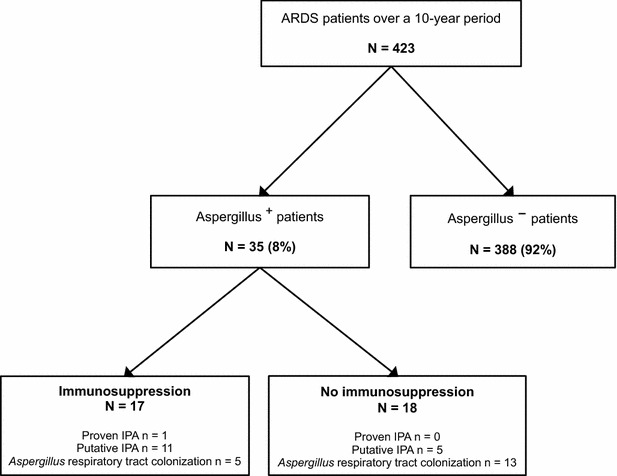
Results: In total, 423 ARDS patients were included with 35 patients [8.3 %, 95 % CI (5.4-10.6)] having at least one respiratory tract sample positive for Aspergillus (Aspergillus(+) patients) after a median delay of 3 days (1-11) following ICU admission. Comorbidities did not differ between Aspergillus(+) and Aspergillus(-) patients except for more frequent immunosuppression in Aspergillus(+) patients (40 vs. 22 %; p = 0.02). There was no difference between Aspergillus(-) and Aspergillus(+) patients regarding in-ICU mortality, ventilator-free days at day 28, and incidence of ventilator-associated pneumonia, but need for renal replacement therapy was higher in Aspergillus(+) patients than in others (49 vs. 27 %; p = 0.01). Seventeen [4.0 %, 95 % CI (2.1-5.9)] patients had putative/proven aspergillosis. After adjusting on covariates associated with ICU mortality, putative/proven aspergillosis was associated with in-ICU mortality [aOR = 9.58 (1.97-46.52); p = 0.005], while Aspergillus colonization was not [aOR = 0.64 (0.21-1.99); p = 0.44].
Conclusions: Eight percent of ARDS patients had Aspergillus spp.-positive respiratory tract cultures. These had a higher risk of mortality only when categorized as having putative or proven invasive pulmonary aspergillosis.
Keywords: Acute respiratory distress syndrome; Aspergillus; Immunosuppression; Invasive pulmonary aspergillosis.
Figures
References
-
- De Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE, Calandra T, Pappas PG, Maertens J, Lortholary O, Kauffman CA, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis. 2008;46:1813–1821. doi: 10.1086/588660. - DOI - PMC - PubMed
-
- Wauters J, Baar I, Meersseman P, Meersseman W, Dams K, De Paep R, Lagrou K, Wilmer A, Jorens P, Hermans G. Invasive pulmonary aspergillosis is a frequent complication of critically ill H1N1 patients: a retrospective study. Intensive Care Med. 2012;38:1761–1768. doi: 10.1007/s00134-012-2673-2. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
