

Clinical Update: Cardiovascular Disease in Diabetes Mellitus: Atherosclerotic Cardiovascular Disease and Heart Failure in Type 2 Diabetes Mellitus - Mechanisms, Management, and Clinical Considerations
- PMID: 27297342
- PMCID: PMC4910510
- DOI: 10.1161/CIRCULATIONAHA.116.022194
Clinical Update: Cardiovascular Disease in Diabetes Mellitus: Atherosclerotic Cardiovascular Disease and Heart Failure in Type 2 Diabetes Mellitus - Mechanisms, Management, and Clinical Considerations
Abstract
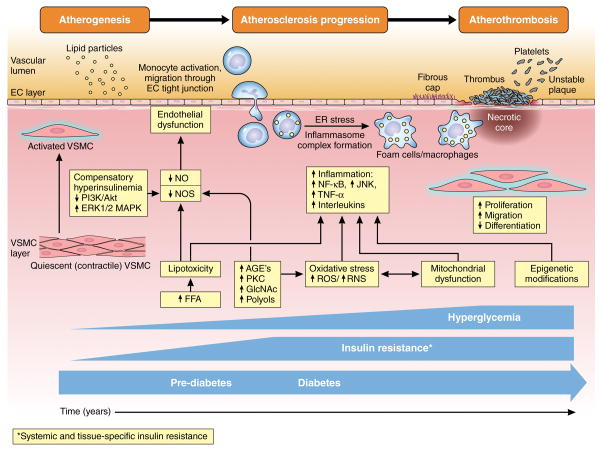
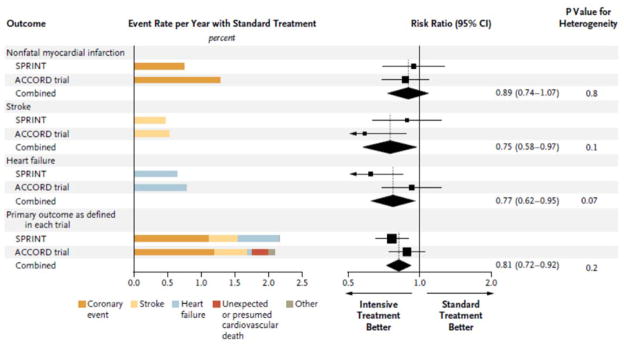
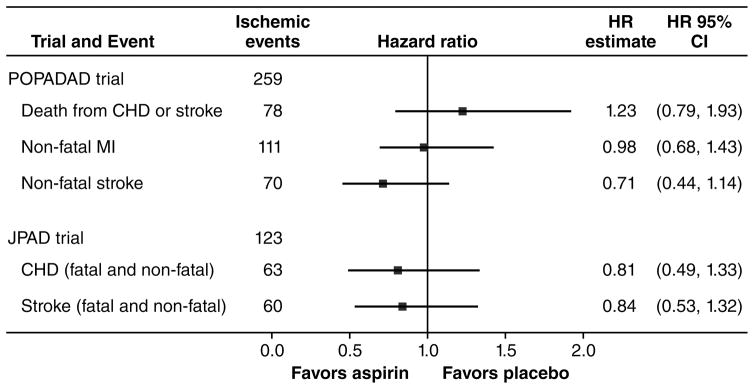
Cardiovascular disease remains the principal cause of death and disability among patients with diabetes mellitus. Diabetes mellitus exacerbates mechanisms underlying atherosclerosis and heart failure. Unfortunately, these mechanisms are not adequately modulated by therapeutic strategies focusing solely on optimal glycemic control with currently available drugs or approaches. In the setting of multifactorial risk reduction with statins and other lipid-lowering agents, antihypertensive therapies, and antihyperglycemic treatment strategies, cardiovascular complication rates are falling, yet remain higher for patients with diabetes mellitus than for those without. This review considers the mechanisms, history, controversies, new pharmacological agents, and recent evidence for current guidelines for cardiovascular management in the patient with diabetes mellitus to support evidence-based care in the patient with diabetes mellitus and heart disease outside of the acute care setting.
Keywords: cardiovascular diseases; diabetes mellitus; drugs; heart failure; trials.
© 2016 American Heart Association, Inc.
Figures
References
-
- Booth GL, Kapral MK, Fung K, Tu JV. Relation between age and cardiovascular disease in men and women with diabetes compared with non-diabetic people: a population-based retrospective cohort study. Lancet. 2006;368:29–36. - PubMed
-
- Beckman JA, Paneni F, Cosentino F, Creager MA. Diabetes and vascular disease: pathophysiology, clinical consequences, and medical therapy: part II. Eur Heart J. 2013;34:2444–2452. - PubMed
-
- World Health Organization. Cardiovascular diseases (CVDs) Fact sheet No 317. [Accessed December 17, 2015];Internet. 2015 Jan; Available at: URL: http://www.who.int/mediacentre/factsheets/fs317/en/
-
- Tancredi M, Rosengren A, Svensson AM, Kosiborod M, Pivodic A, Gudbjornsdottir S, Wedel H, Clements M, Dahlqvist S, Lind M. Excess Mortality among Persons with Type 2 Diabetes. N Engl J Med. 2015;373:1720–1732. - PubMed
-
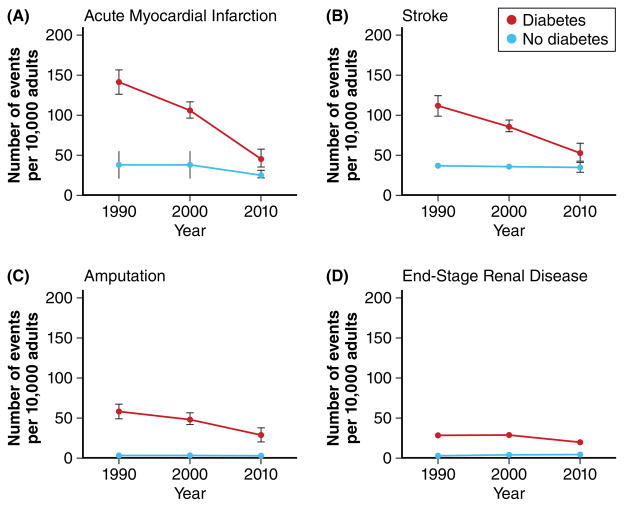
- Gregg EW, Li Y, Wang J, Burrows NR, Ali MK, Rolka D, Williams DE, Geiss L. Changes in diabetes-related complications in the United States, 1990–2010. N Engl J Med. 2014;370:1514–1523. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
