

Perforation in an intestinal malignant lymphoma case
- PMID: 27297406
- PMCID: PMC4906586
- DOI: 10.1186/s13104-016-2111-6
Perforation in an intestinal malignant lymphoma case
Abstract
Background: The gastrointestinal tract is a relatively common involvement site in lymphoma and, in such cases, intestinal perforation is a concern before and during chemotherapy. The prediction of intestinal perforation prior to chemotherapy is difficult, and there is no standard strategy to minimize the frequency of severely adverse gastrointestinal events in lymphoma cases.
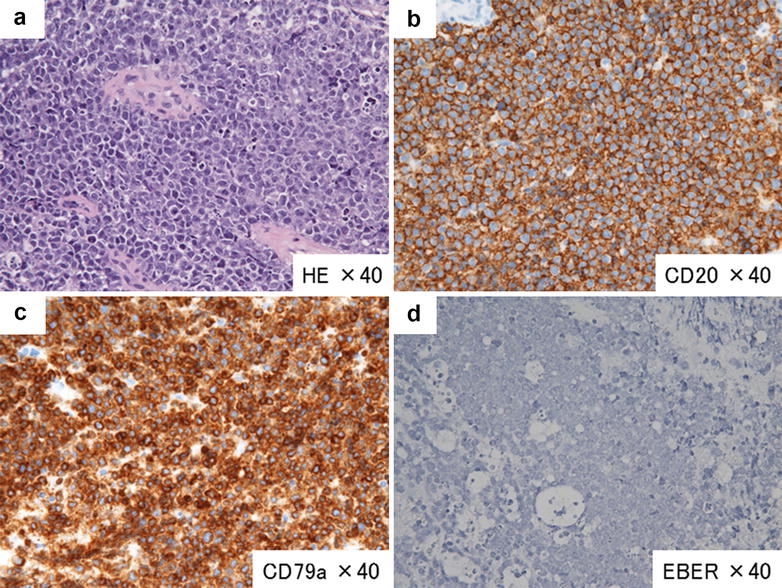
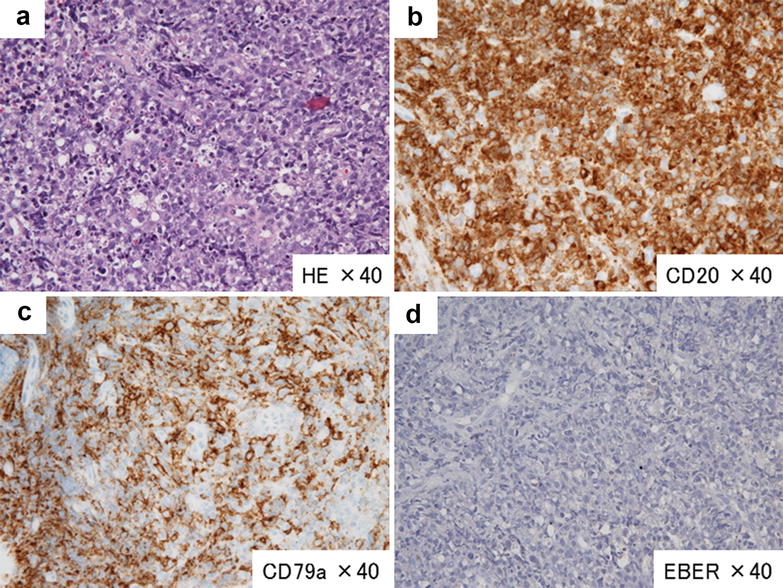
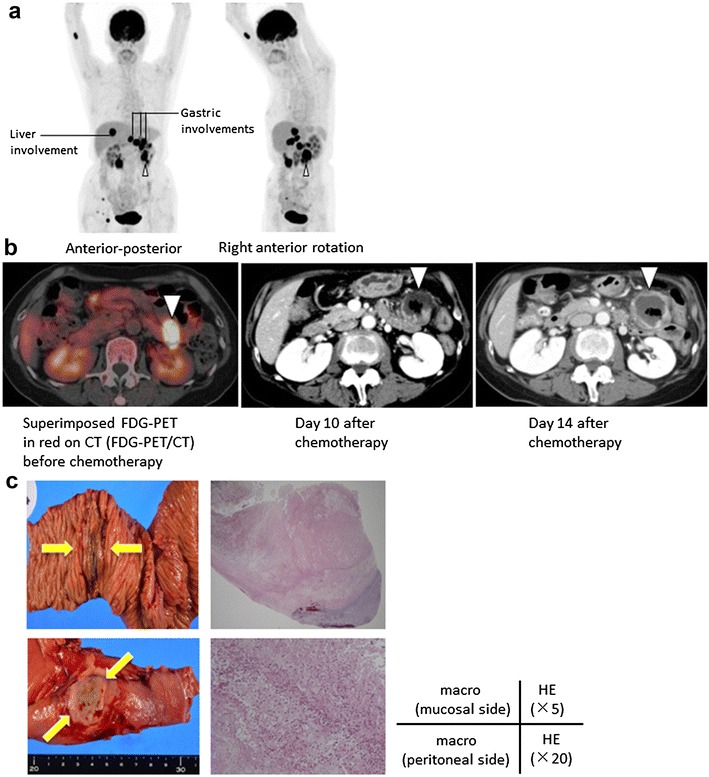
Case presentation: The 61-year-old female patient had a history of primary central nervous system lymphoma (PCNSL), diagnosed histologically as diffuse large B cell lymphoma (DLBCL). We administered six courses of intensive chemotherapy consisting of high-dose methotrexate and sequential whole-brain irradiation (40.5 Gy). After a 3-year remission of the PCNSL, the patient's lymphoma recurred, involving the small intestine. (18)F-FDG-PET/CT upon the recurrence before chemotherapy showed multiple nodular lesions in the patient's gastrointestinal tract. Central nervous system lesions were not detected. We administered intensive salvage chemotherapy consisting of cyclophosphamide, high-dose AraC, methyl-prednisolone, etoposide, and rituximab. The response was a rapid partial response, but on day 10 after the initiation of salvage chemotherapy, she complained of abdominal pain with tenderness. The contrast-enhanced (CE)-CT revealed transmural ischemia of the intestine. On the 7th day after the onset of urgent abdominal symptoms, follow-up CE-CT showed that the ischemic lesion had become thin. We conducted elective surgery after waiting for the complete recovery of the patient's white blood cell count. The pathological findings of resected intestine confirmed the elimination of the majority of lymphoma cells and concomitant partial necrotic tissue.
Conclusions: We were able to avoid the neutropenic period and safely conducted the surgical treatment for the subclinical perforation by using CE-CT. The combination of (18)F-FDG-PET/CT before chemotherapy and CE-CT scanning for the targeted involvement site helped us evaluate the surgical indications and optimal timing of surgery in a lymphoma patient with gastrointestinal involvement.
Keywords: Chemotherapy; Malignant lymphoma; Perforation.
Figures
References
-
- Gobbi PG, Ghirardelli ML, Cavalli C, et al. The role of surgery in the treatment of gastrointestinal lymphomas other than low-grade MALT lymphomas. Haematologica. 2000;85:372–380. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
