

Disparities in achieving and sustaining viral suppression among a large cohort of HIV-infected persons in care - Washington, DC
- PMID: 27297952
- PMCID: PMC5084086
- DOI: 10.1080/09540121.2016.1189496
Disparities in achieving and sustaining viral suppression among a large cohort of HIV-infected persons in care - Washington, DC
Abstract
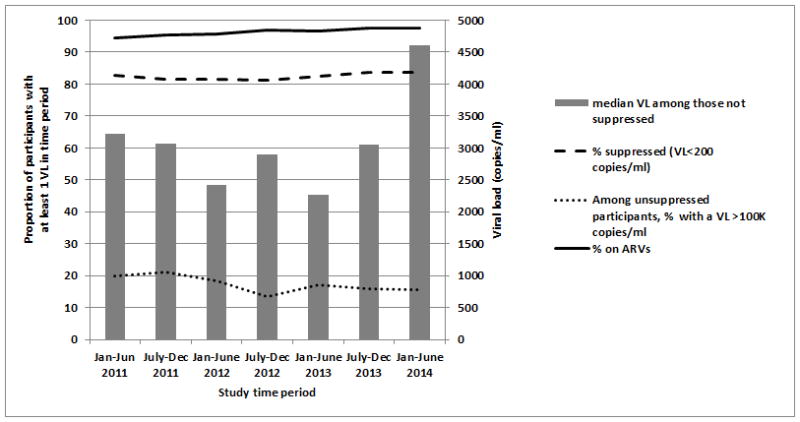
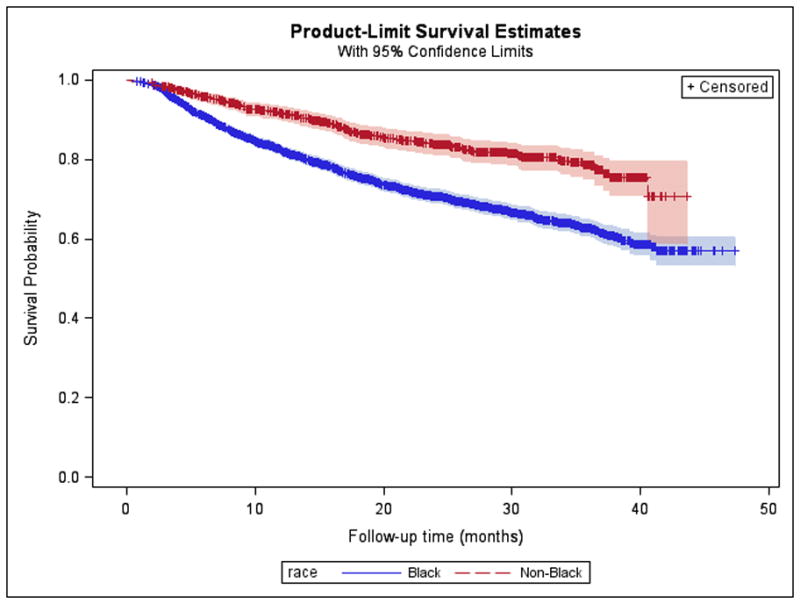
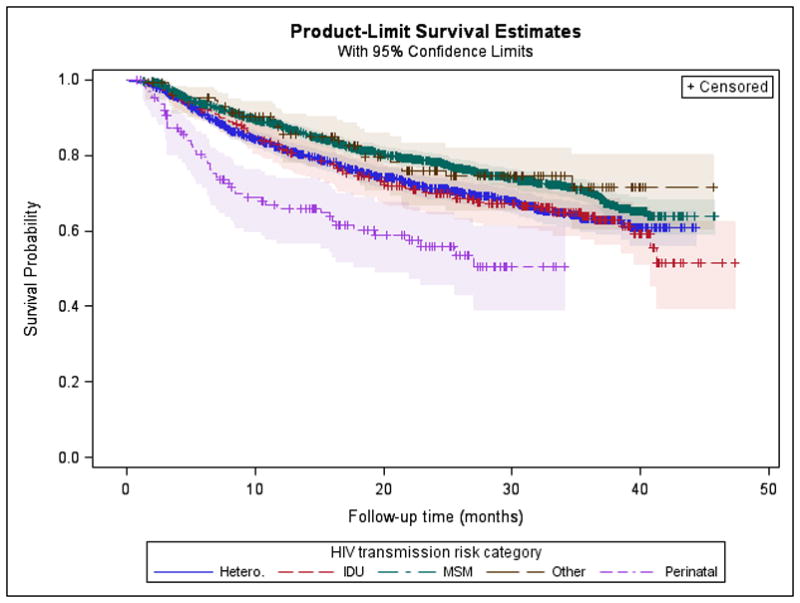
One goal of the HIV care continuum is achieving viral suppression (VS), yet disparities in suppression exist among subpopulations of HIV-infected persons. We sought to identify disparities in both the ability to achieve and sustain VS among an urban cohort of HIV-infected persons in care. Data from HIV-infected persons enrolled at the 13 DC Cohort study clinical sites between January 2011 and June 2014 were analyzed. Univariate and multivariate logistic regression were conducted to identify factors associated with achieving VS (viral load < 200 copies/ml) at least once, and Kaplan-Meier (KM) curves and Cox proportional hazards models were used to identify factors associated with sustaining VS and time to virologic failure (VL ≥ 200 copies/ml after achievement of VS). Among the 4311 participants, 95.4% were either virally suppressed at study enrollment or able to achieve VS during the follow-up period. In multivariate analyses, achieving VS was significantly associated with age (aOR: 1.04; 95%CI: 1.03-1.06 per five-year increase) and having a higher CD4 (aOR: 1.05, 95% CI 1.04-1.06 per 100 cells/mm(3)). Patients infected through perinatal transmission were less likely to achieve VS compared to MSM patients (aOR: 0.63, 95% CI 0.51-0.79). Once achieved, most participants (74.4%) sustained VS during follow-up. Blacks and perinatally infected persons were less likely to have sustained VS in KM survival analysis (log rank chi-square p ≤ .001 for both) compared to other races and risk groups. Earlier time to failure was observed among females, Blacks, publically insured, perinatally infected, those with longer standing HIV infection, and those with diagnoses of mental health issues or depression. Among this HIV-infected cohort, most people achieved and maintained VS; however, disparities exist with regard to patient age, race, HIV transmission risk, and co-morbid conditions. Identifying populations with disparate outcomes allows for appropriate targeting of resources to improve outcomes along the care continuum.
Keywords: HIV; Viral suppression; care continuum; cohort; disparities.
Conflict of interest statement
The authors have no conflicts to declare.
Figures
References
-
- Anastos K, Gange SJ, Lau B, Weiser B, Detels R, Giorgi JV, … Greenblatt RM. Association of race and gender with HIV-1 RNA levels and immunologic progression. J Acquir Immune Defic Syndr. 2000;24(3):218–226. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials