

What are the most efficacious treatment regimens for isoniazid-resistant tuberculosis? A systematic review and network meta-analysis
- PMID: 27298314
- PMCID: PMC5036252
- DOI: 10.1136/thoraxjnl-2015-208262
What are the most efficacious treatment regimens for isoniazid-resistant tuberculosis? A systematic review and network meta-analysis
Abstract
Introduction: Consensus on the best treatment regimens for patients with isoniazid-resistant TB is limited; global treatment guidelines differ. We undertook a systematic review and meta-analysis using mixed-treatment comparisons methodology to provide an up-to-date summary of randomised controlled trials (RCTs) and relative regimen efficacy.
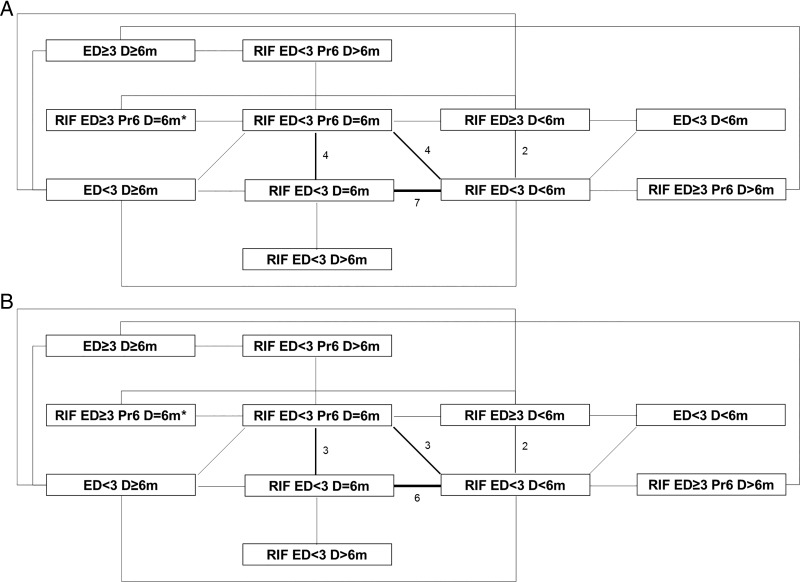
Methods: Ovid MEDLINE, the Web of Science and EMBASE were mined using search terms for TB, drug therapy and RCTs. Extracted data were inputted into fixed-effects and random-effects models. ORs for all possible network comparisons and hierarchical rankings for different regimens were obtained.
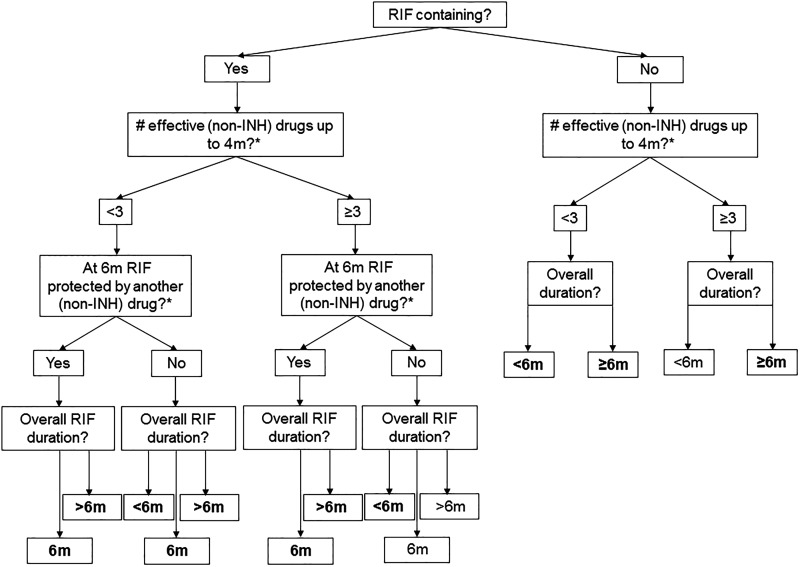
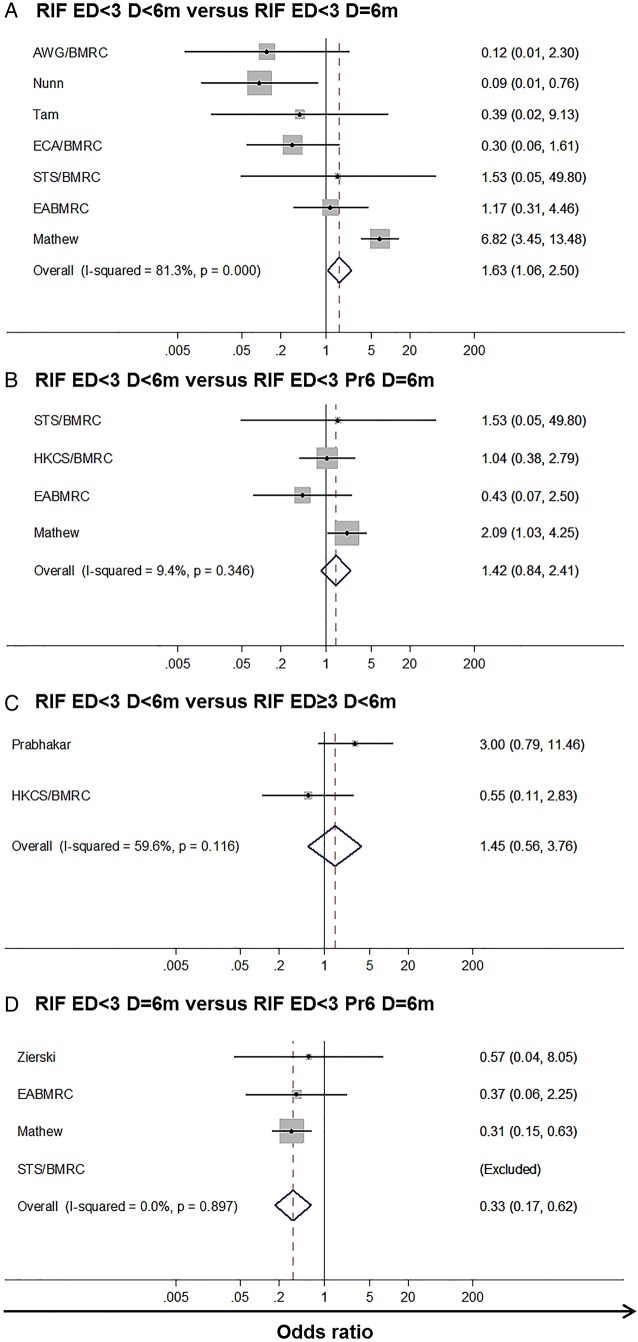
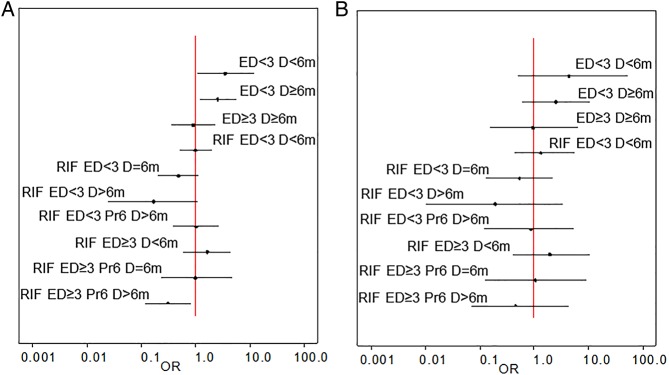
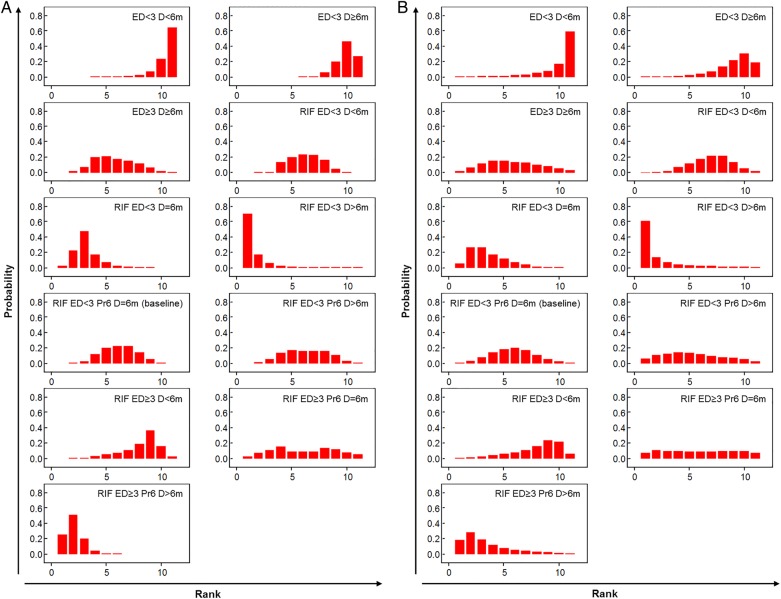
Results: 12 604 records were retrieved and 118 remained postextraction, representing 59 studies-27 standalone and 32 with multiple papers. In comparison to a baseline category that included the WHO-recommended regimen for countries with high levels of isoniazid resistance (rifampicin-containing regimens using fewer than three effective drugs at 4 months, in which rifampicin was protected by another effective drug at 6 months, and rifampicin was taken for 6 months), extending the duration of rifampicin and increasing the number of effective drugs at 4 months lowered the odds of unfavourable outcomes (treatment failure or the lack of microbiological cure; relapse post-treatment; death due to TB) in a fixed-effects model (OR 0.31 (95% credible interval 0.12-0.81)). In a random-effects model all estimates crossed the null.
Conclusions: Our systematic review and network meta-analysis highlight a regimen category that may be more efficacious than the WHO population level recommendation, and identify knowledge gaps where data are sparse.
Systematic review registration number: PROSPERO CRD42014015025.
Keywords: Clinical Epidemiology; Tuberculosis.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
Similar articles
-
Six-month therapy for abdominal tuberculosis.Cochrane Database Syst Rev. 2016 Nov 1;11(11):CD012163. doi: 10.1002/14651858.CD012163.pub2. Cochrane Database Syst Rev. 2016. PMID: 27801499 Free PMC article.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2021 Apr 19;4(4):CD011535. doi: 10.1002/14651858.CD011535.pub4. Cochrane Database Syst Rev. 2021. Update in: Cochrane Database Syst Rev. 2022 May 23;5:CD011535. doi: 10.1002/14651858.CD011535.pub5. PMID: 33871055 Free PMC article. Updated.
-
Xpert® MTB/RIF assay for extrapulmonary tuberculosis and rifampicin resistance.Cochrane Database Syst Rev. 2018 Aug 27;8(8):CD012768. doi: 10.1002/14651858.CD012768.pub2. Cochrane Database Syst Rev. 2018. Update in: Cochrane Database Syst Rev. 2021 Jan 15;1:CD012768. doi: 10.1002/14651858.CD012768.pub3. PMID: 30148542 Free PMC article. Updated.
-
Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis.Cochrane Database Syst Rev. 2017 Dec 22;12(12):CD011535. doi: 10.1002/14651858.CD011535.pub2. Cochrane Database Syst Rev. 2017. Update in: Cochrane Database Syst Rev. 2020 Jan 9;1:CD011535. doi: 10.1002/14651858.CD011535.pub3. PMID: 29271481 Free PMC article. Updated.
-
Drugs for preventing postoperative nausea and vomiting in adults after general anaesthesia: a network meta-analysis.Cochrane Database Syst Rev. 2020 Oct 19;10(10):CD012859. doi: 10.1002/14651858.CD012859.pub2. Cochrane Database Syst Rev. 2020. PMID: 33075160 Free PMC article.
Cited by
-
Isoniazid Monoresistance and Rate of Culture Conversion among Patients in the State of Georgia with Confirmed Tuberculosis, 2009-2014.Ann Am Thorac Soc. 2018 Mar;15(3):331-340. doi: 10.1513/AnnalsATS.201702-147OC. Ann Am Thorac Soc. 2018. PMID: 29131662 Free PMC article.
-
Isoniazid-monoresistant tuberculosis is associated with poor treatment outcomes in Durban, South Africa.Int J Tuberc Lung Dis. 2017 Jun 1;21(6):670-676. doi: 10.5588/ijtld.16.0843. Int J Tuberc Lung Dis. 2017. PMID: 28482962 Free PMC article.
-
Evaluation of Anyplex™ II MTB/MDR kit's performance to rapidly detect isoniazid and rifampicin resistant Mycobacterium tuberculosis from various clinical specimens.Mol Biol Rep. 2020 Apr;47(4):2501-2508. doi: 10.1007/s11033-020-05331-8. Epub 2020 Mar 2. Mol Biol Rep. 2020. PMID: 32124172
-
Treatment of Isoniazid-Resistant Pulmonary Tuberculosis.Tuberc Respir Dis (Seoul). 2020 Jan;83(1):20-30. doi: 10.4046/trd.2019.0065. Tuberc Respir Dis (Seoul). 2020. PMID: 31905429 Free PMC article. Review.
-
Isoniazid-resistant tuberculosis: a cause for concern?Int J Tuberc Lung Dis. 2017 Feb 1;21(2):129-139. doi: 10.5588/ijtld.16.0716. Int J Tuberc Lung Dis. 2017. PMID: 28234075 Free PMC article. Review.
References
-
- World Health Organization. Global tuberculosis report 2015. 2015. http://www.who.int/tb/publications/global_report/en/ (accessed 2 Nov 2015).
-
- World Health Organization. Treatment of tuberculosis: guidelines. 4th edn 2009. http://www.who.int/tb/publications/2010/9789241547833/en/ (accessed 7 Jan 2013).
-
- World Health Organization. Companion handbook to the WHO guidelines for the programmatic management of drug-resistant tuberculosis. 2014. http://www.who.int/tb/publications/pmdt_companionhandbook/en/ (accessed 8 Mar 2016). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical