

Effect of Pathologic Tumor Response and Nodal Status on Survival in the Medical Research Council Adjuvant Gastric Infusional Chemotherapy Trial
- PMID: 27298411
- PMCID: PMC5019747
- DOI: 10.1200/JCO.2015.65.7692
Effect of Pathologic Tumor Response and Nodal Status on Survival in the Medical Research Council Adjuvant Gastric Infusional Chemotherapy Trial
Abstract
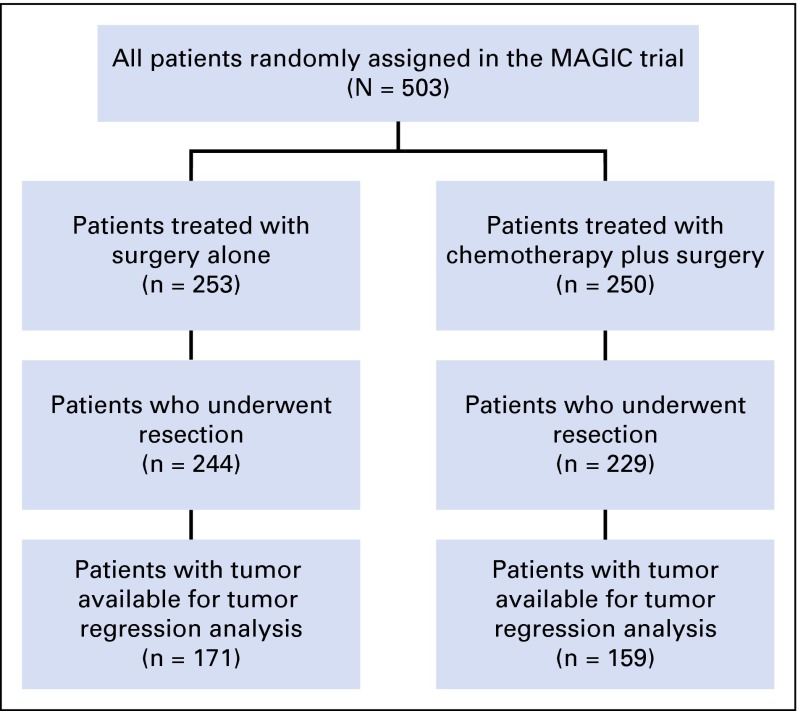
Purpose: The Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial established perioperative epirubicin, cisplatin, and fluorouracil chemotherapy as a standard of care for patients with resectable esophagogastric cancer. However, identification of patients at risk for relapse remains challenging. We evaluated whether pathologic response and lymph node status after neoadjuvant chemotherapy are prognostic in patients treated in the MAGIC trial.
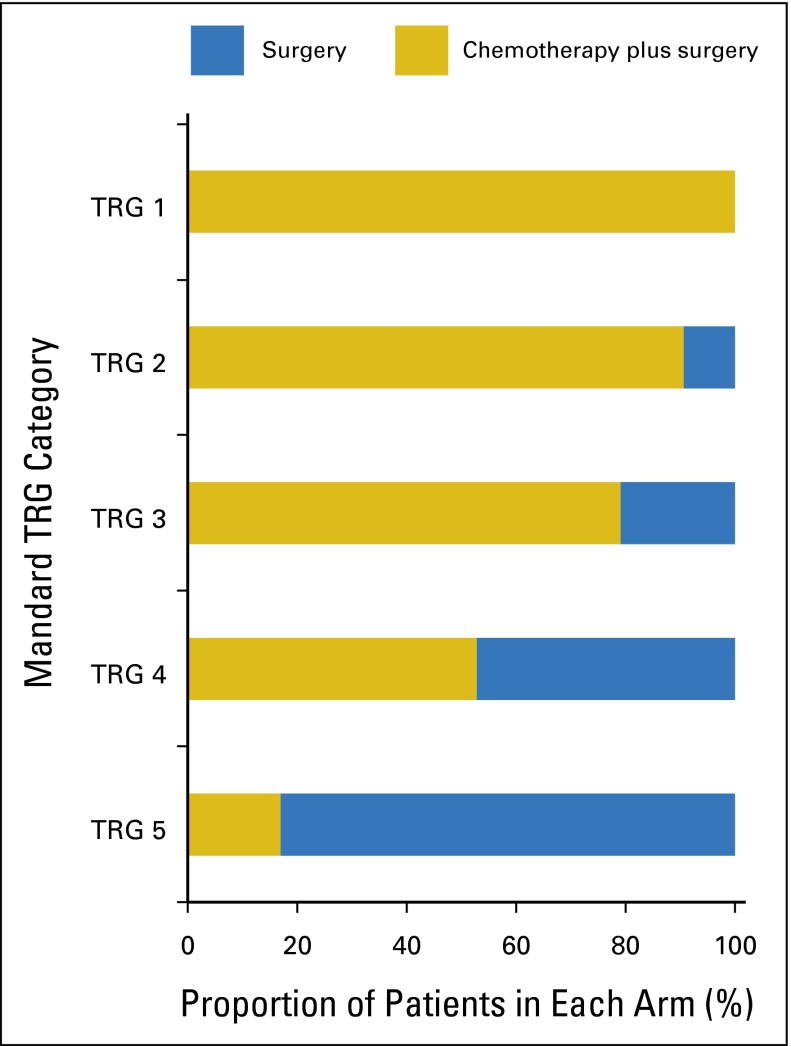
Materials and methods: Pathologic regression was assessed in resection specimens by two independent pathologists using the Mandard tumor regression grading system (TRG). Differences in overall survival (OS) according to TRG were assessed using the Kaplan-Meier method and compared using the log-rank test. Univariate and multivariate analyses using the Cox proportional hazards method established the relationships among TRG, clinical-pathologic variables, and OS.
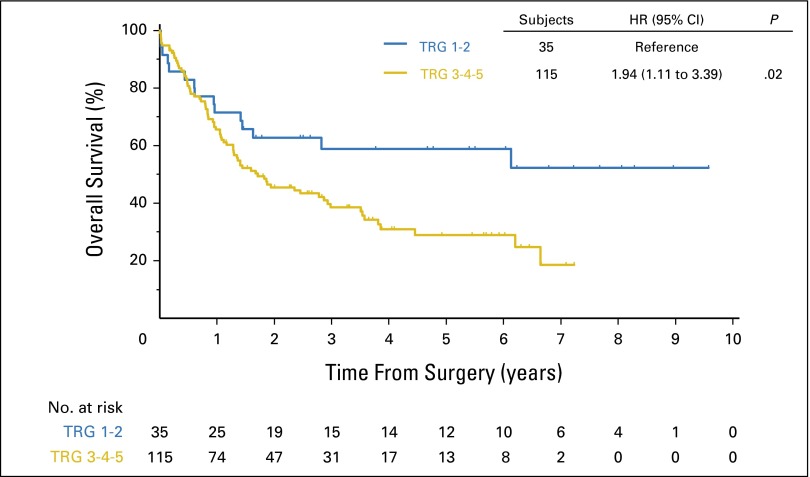
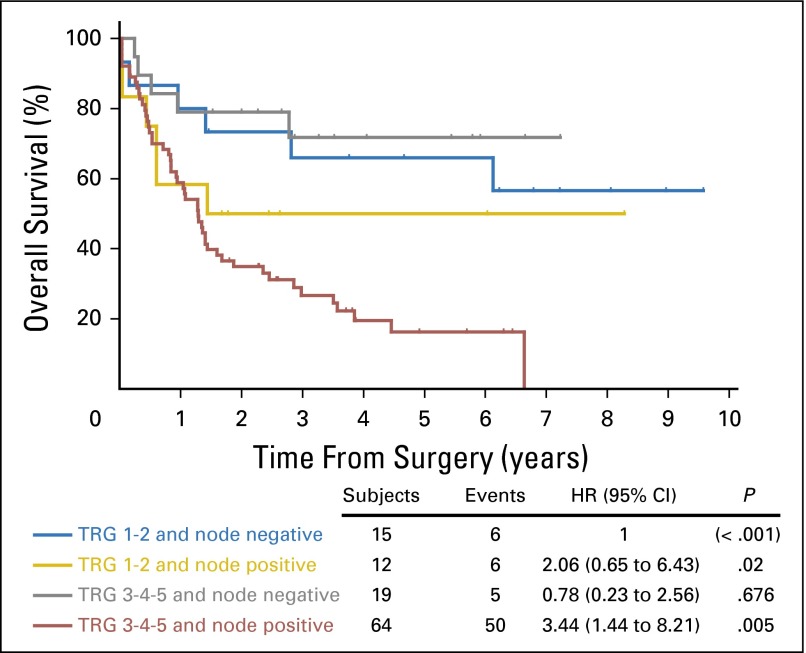
Results: Three hundred thirty resection specimens were analyzed. In chemotherapy-treated patients with a TRG of 1 or 2, median OS was not reached, whereas for patients with a TRG of 3, 4, or 5, median OS was 20.47 months. On univariate analysis, high TRG and lymph node metastases were negatively related to survival (Mandard TRG 3, 4, or 5: hazard ratio [HR], 1.94; 95% CI, 1.11 to 3.39; P = .0209; lymph node metastases: HR, 3.63; 95% CI, 1.88 to 7.0; P < .001). On multivariate analysis, only lymph node status was independently predictive of OS (HR, 3.36; 95% CI, 1.70 to 6.63; P < .001).
Conclusion: Lymph node metastases and not pathologic response to chemotherapy was the only independent predictor of survival after chemotherapy plus resection in the MAGIC trial. Prospective evaluation of whether omitting postoperative chemotherapy and/or switching to a noncross-resistant regimen in patients with lymph node-positive disease whose tumor did not respond to preoperative epirubicin, cisplatin, and fluorouracil may be appropriate.
© 2016 by American Society of Clinical Oncology.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest are found in the article online at www.jco.org. Author contributions are found at the end of this article.
Figures
Comment in
-
Impact of pathologic tumor response in the treatment of gastric cancer.Transl Gastroenterol Hepatol. 2016 Sep 21;1:71. doi: 10.21037/tgh.2016.09.04. eCollection 2016. Transl Gastroenterol Hepatol. 2016. PMID: 28138637 Free PMC article. No abstract available.
-
Pathologic tumor response to neoadjuvant chemotherapy in gastroesophageal cancer: what does it mean?Transl Gastroenterol Hepatol. 2016 Sep 23;1:75. doi: 10.21037/tgh.2016.09.08. eCollection 2016. Transl Gastroenterol Hepatol. 2016. PMID: 28138641 Free PMC article. No abstract available.
References
-
- Medical Research Council Oesophageal Cancer Working Group Surgical resection with or without preoperative chemotherapy in oesophageal cancer: A randomised controlled trial. Lancet. 2002;359:1727–1733. - PubMed
-
- Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11–20. - PubMed
-
- van Hagen P, Hulshof MCCM, van Lanschot JJB, et al. Preoperative chemoradiotherapy for esophageal or junctional cancer. N Engl J Med. 2012;366:2074–2084. - PubMed
-
- Ychou M, Boige V, Pignon J-P, et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: An FNCLCC and FFCD multicenter phase III trial. J Clin Oncol. 2011;29:1715–1721. - PubMed
-
- Kattan MW, Karpeh MS, Mazumdar M, et al. Postoperative nomogram for disease-specific survival after an R0 resection for gastric carcinoma. J Clin Oncol. 2003;21:3647–3650. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
