

Avascular Necrosis of Acetabulum: The Hidden Culprit of Resistant Deep Wound Infection and Failed Fixation of Fracture Acetabulum - A Case Report
- PMID: 27299095
- PMCID: PMC4845453
- DOI: 10.13107/jocr.2250-0685.341
Avascular Necrosis of Acetabulum: The Hidden Culprit of Resistant Deep Wound Infection and Failed Fixation of Fracture Acetabulum - A Case Report
Abstract
Introduction: Chances of avascular necrosis of acetabulum are rare as it enjoys a rich blood supply. But cases of post - traumatic avascular necrosis of acetabulum following fracture of posterior column have been well documented. Importance of identifying and suspecting the avascular necrosis of acetabulum is essential in cases of failed fixation of fracture acetabulum, previously operated using extensile approach to acetabulum; either extended anterior ilio - femoral or tri - radiate approach. Such patients usually present with repeated deep bone infection or with early failure of fixation with aseptic loosening and migration of its components. We present a similar case.
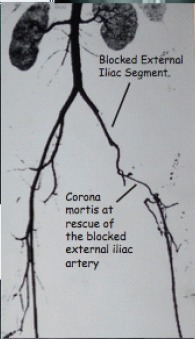
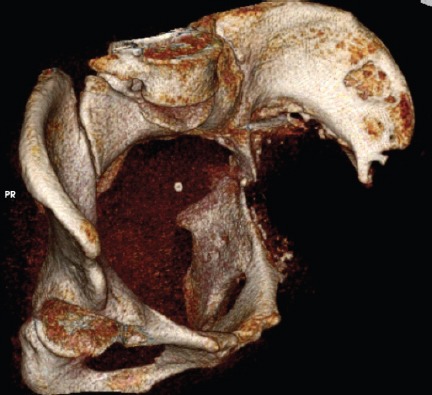
Case presentation: 40 years female presented with inadequately managed transverse fracture of left acetabulum done by anterior extended ilio-inguinal approach. The fixation failed. She presented 6 months later with painful hip. Cemented total hip replacement was performed with reconstruction of acetabulum by posterior column plating. Six months postoperatively patient presented with dislodgement of cup, pelvic discontinuity and sinus in the thigh. Two stage revision surgery was planned. First implant, removal; debridement and antibiotic spacer surgery was performed. At second stage of revision total hip replacement, patient had Paprosky grade IIIb defect in acetabulum. Spacer was removed through the posterior approach. Anterior approach was taken for anterior plating. Intra-operatively external iliac pulsations were found to be absent so procedure was abandoned after expert opinion. Postoperatively digital subtraction angiography demonstrated a chronic block in the external iliac artery and corona mortis was the only patent vascular channel providing vascular to the left lower limb. Thus, peripheral limb was stealing blood supply from the acetabulum to maintain perfusion. Patient was ultimately left with pelvic discontinuity, excision arthroplasty and pseudoarthrosis of the left hip.
Conclusions: Avascular necrosis of acetabulum is a rare entity & often not recognized. One should be suspicious about diagnosis of avascular necrosis of acetabulum in select cases of failed acetabular fixation, previously operated via extensile anterior ilio - inguinal approach. Angiographic evaluation is essential in revision cases of failed acetabular fixation. Corona mortis (crown or circle of death) can sometimes act as a savior of limb.
Keywords: Avascular Necrosis Acetabulum; Corona Mortis; Pelvic Discontinuity.
Conflict of interest statement
Conflict of Interest: Nil
Figures








References
-
- Itokazu M, Takahashi K, Matsunaga T, Hayakawa D, Emura S, Isono H, et al. A study of the arterial supply of the human acetabulum using a corrosion casting method. Clin Anat. 1997;10(2):77–81. - PubMed
-
- LetourneI E, Judet R, editors. Fractures of the Acetabulum. ed 2. New York, NY: Springer-Verlag; 1993. p. 545.
-
- Judet R. Les fractures du cotyle. ActalOrthopBelge. 1966;32:469–476. - PubMed
-
- Mears D. Avascular necrosis of the acetabulum. Operative techniques in orthopaedics. 1997 Jul 7;(No. 3)
-
- Paprosky WG, Magrus RE. Principles of bone grafting in revision total hip arthroplasty: Acetabular techniques. ClinOrthop. 1994;298:147–155. - PubMed
Publication types
LinkOut - more resources
Full Text Sources