

Prescription of Long-Acting Opioids and Mortality in Patients With Chronic Noncancer Pain
- PMID: 27299617
- PMCID: PMC5030814
- DOI: 10.1001/jama.2016.7789
Prescription of Long-Acting Opioids and Mortality in Patients With Chronic Noncancer Pain
Abstract
Importance: Long-acting opioids increase the risk of unintentional overdose deaths but also may increase mortality from cardiorespiratory and other causes.
Objective: To compare all-cause mortality for patients with chronic noncancer pain who were prescribed either long-acting opioids or alternative medications for moderate to severe chronic pain.
Design, setting, and participants: Retrospective cohort study between 1999 and 2012 of Tennessee Medicaid patients with chronic noncancer pain and no evidence of palliative or end-of-life care.
Exposures: Propensity score-matched new episodes of prescribed therapy for long-acting opioids or either analgesic anticonvulsants or low-dose cyclic antidepressants (control medications).
Main outcomes and measures: Total and cause-specific mortality as determined from death certificates. Adjusted hazard ratios (HRs) and risk differences (difference in incidence of death) were calculated for long-acting opioid therapy vs control medication.
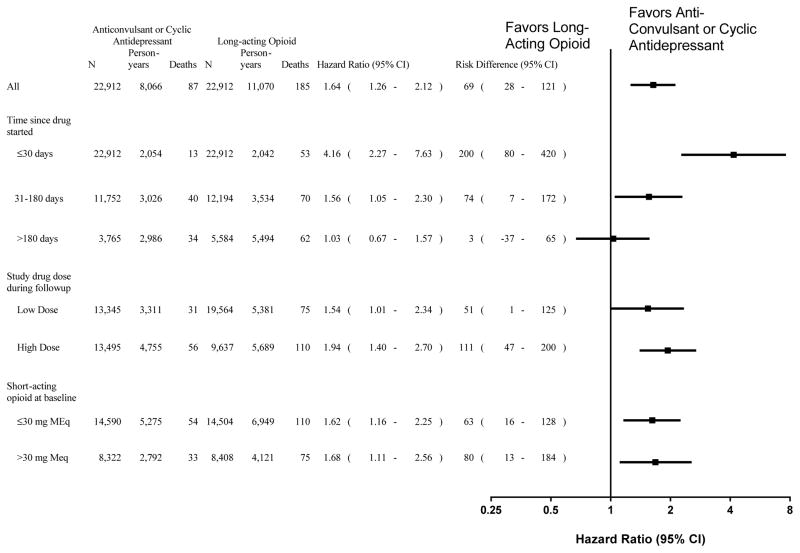
Results: There were 22,912 new episodes of prescribed therapy for both long-acting opioids and control medications (mean [SD] age, 48 [11] years; 60% women). The long-acting opioid group was followed up for a mean 176 days and had 185 deaths and the control treatment group was followed up for a mean 128 days and had 87 deaths. The HR for total mortality was 1.64 (95% CI, 1.26-2.12) with a risk difference of 68.5 excess deaths (95% CI, 28.2-120.7) per 10,000 person-years. Increased risk was due to out-of-hospital deaths (154 long-acting opioid, 60 control deaths; HR, 1.90; 95% CI, 1.40-2.58; risk difference, 67.1; 95% CI, 30.1-117.3) excess deaths per 10,000 person-years. For out-of-hospital deaths other than unintentional overdose (120 long-acting opioid, 53 control deaths), the HR was 1.72 (95% CI, 1.24-2.39) with a risk difference of 47.4 excess deaths (95% CI, 15.7-91.4) per 10,000 person-years. The HR for cardiovascular deaths (79 long-acting opioid, 36 control deaths) was 1.65 (95% CI, 1.10-2.46) with a risk difference of 28.9 excess deaths (95% CI, 4.6-65.3) per 10,000 person-years. The HR during the first 30 days of therapy (53 long-acting opioid, 13 control deaths) was 4.16 (95% CI, 2.27-7.63) with a risk difference of 200 excess deaths (95% CI, 80-420) per 10,000 person-years.
Conclusions and relevance: Prescription of long-acting opioids for chronic noncancer pain, compared with anticonvulsants or cyclic antidepressants, was associated with a significantly increased risk of all-cause mortality, including deaths from causes other than overdose, with a modest absolute risk difference. These findings should be considered when evaluating harms and benefits of treatment.
Conflict of interest statement
Disclosures: All authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported.
Figures
Comment in
-
Long acting opioids are linked to increased risk of death.BMJ. 2016 Jun 14;353:i3313. doi: 10.1136/bmj.i3313. BMJ. 2016. PMID: 27307304 No abstract available.
References
-
- Okie S. A flood of opioids, a rising ride of deaths. N Engl J Med. 2010;363:1981–1985. - PubMed
-
- Vital signs: overdoses of prescription opioid pain relievers---United States, 1999–2008. MMWR Morb Mortal Wkly Rep. 2011;60:1487–1492. - PubMed
-
- Bohnert ASB, Valenstein M, Bair MJ, et al. Association between opioid prescribing patterns and opioid overdose-related deaths. JAMA. 2011;305:1315–1321. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
