

Glycemic Control, Renal Complications, and Current Smoking in Relation to Excess Risk of Mortality in Persons With Type 1 Diabetes
- PMID: 27301980
- PMCID: PMC5032961
- DOI: 10.1177/1932296816652901
Glycemic Control, Renal Complications, and Current Smoking in Relation to Excess Risk of Mortality in Persons With Type 1 Diabetes
Abstract
Background: A substantial excess risk of mortality still exists in persons with type 1 diabetes. The aim of this study was to evaluate the excess risk of mortality in persons with type 1 diabetes without renal complications who target goals for glycemic control and are nonsmokers. Furthermore, we evaluated risk factors of death due to hypoglycemia or ketoacidosis in young adults with type 1 diabetes.
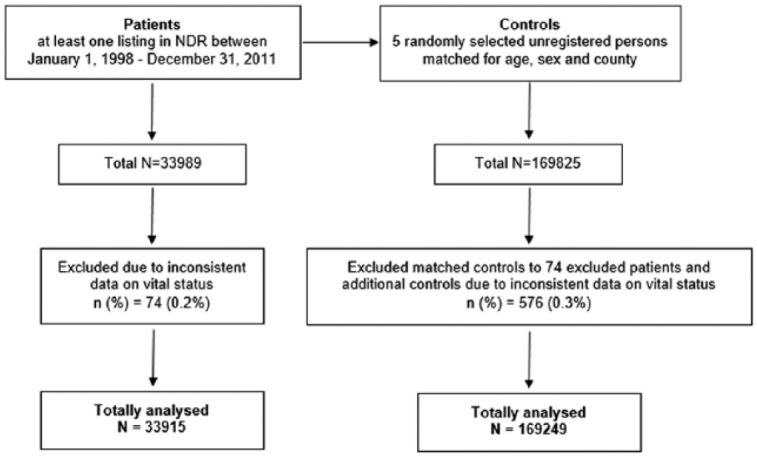
Methods: We evaluated a cohort based on 33 915 persons with type 1 diabetes and 169 249 randomly selected controls from the general population matched on age, sex, and county followed over a mean of 8.0 and 8.3 years, respectively. Hazard ratios (HRs) for all-cause and cardiovascular disease (CVD) mortality for persons with type 1 diabetes versus controls were estimated.
Results: The adjusted HRs for all-cause and CVD mortality for persons with type 1 diabetes without renal complications (normoalbuminuria and eGFR ≥ 60 ml/min) and HbA1c ≤ 6.9% (52 mmol/mol) compared to controls were 1.22 (95% CI 0.98-1.52) and 1.03 (95% CI 0.66-1.60), respectively. The HRs increased with higher updated mean HbA1c. For nonsmokers in this group, the HRs for all-cause and CVD mortality were somewhat lower: 1.11 (95% CI 0.87-1.42) and 0.89 (95% CI 0.53-1.48) at updated mean HbA1c ≤ 6.9% (52 mmol/mol). HRs for significant predictors for deaths due to hypoglycemia or ketoacidosis in persons < 50 years were male sex 2.40 (95% CI 1.27-4.52), smoking 2.86 (95% CI 1.57-5.22), lower educational level 3.01 (95% CI 1.26-7.22), albuminuria or advanced kidney disease 2.83 (95% CI 1.63-4.93), earlier hospital diagnosis of hypoglycemia or ketoacidosis 2.30 (95% CI 1.20-4.42), and earlier diagnosis of intoxication 2.53 (95% CI 1.06-6.04).
Conclusions: If currently recommended HbA1c targets can be reached, renal complications and smoking avoided in persons with type 1 diabetes, the excess risk of mortality will likely converge substantially to that of the general population.
Keywords: hypoglycemia; ketoacidosis; mortality; type 1 diabetes mellitus.
© 2016 Diabetes Technology Society.
Conflict of interest statement
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: ML reports receiving honoraria or having been a consultant for AstraZeneca, Eli Lilly, Medtronic, Novo Nordisk, and Pfizer and grant support from Abbott, AstraZeneca, Dexcom, Novo Nordisk, and Pfizer. All other authors declare no conflicts of interest.
References
-
- American Diabetes Association. Standards of medical care in diabetes—2014. Diabetes Care. 2014;37(suppl 1):S14-S80. - PubMed
-
- Type 1 diabetes: diagnosis and management of type 1 diabetes in children, young people and adults. Available at: http://egap.evidence.nhs.uk/type-1-diabetes-cg15/guidance#blood-glucose-.... Accessed January 8, 2014.
-
- Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes. 2013;37(suppl 1):S1-S212. - PubMed
-
- Lind M, Svensson AM, Kosiborod M, et al. Glycemic control and excess mortality in type 1 diabetes. N Engl J Med. 2014;371(21):1972-1982. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
