

Operative management of locally advanced, differentiated thyroid cancer
- PMID: 27302105
- PMCID: PMC5126966
- DOI: 10.1016/j.surg.2016.04.027
Operative management of locally advanced, differentiated thyroid cancer
Abstract
Background: The majority of differentiated thyroid cancer tends to present with limited locoregional disease, leading to excellent long-term survival after operative treatment. Even patients with advanced local disease may survive for long periods with appropriate treatment. The aim of this study is to present our institutional experience of the management of locally advanced differentiated thyroid cancer and to analyze factors predictive of outcome.
Methods: We reviewed our institutional database of 3,664 previously untreated patients with differentiated thyroid cancer operated between 1986 and 2010. A total of 153 patients had tumor extension beyond the thyroid capsule that invaded the subcutaneous soft tissues, recurrent laryngeal nerve, larynx, trachea, or esophagus. Details on extent of operation and adjuvant therapy were recorded. Disease-specific survival and locoregional recurrence-free probability were determined by the Kaplan-Meier method. Factors predictive of outcome were determined by multivariate analysis.
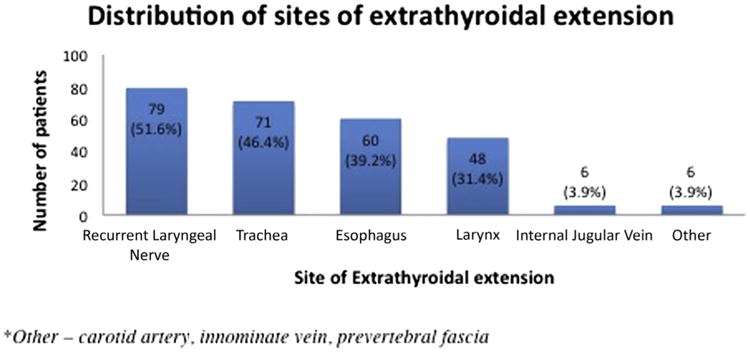
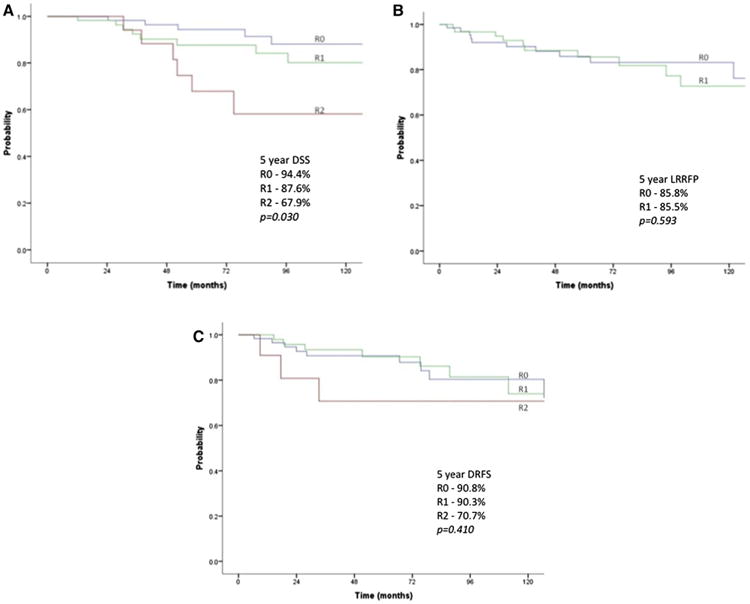
Results: The median age of the 153 patients with tumor extension beyond the thyroid capsule was 55 years (range 11-91 years). Eighty-nine patients (58.2%) were female. Twenty-three patients (15.0%) were staged as M1 at presentation, and 122 (79.7%) had pathologically involved lymph nodes. The most common site of extrathyroidal extension was the recurrent laryngeal nerve (51.0%) followed by the trachea (46.4%) and esophagus (39.2%). Sixty-three patients (41%) required resection of the recurrent laryngeal nerve due to tumor involvement. After surgery, 20 patients (13.0%) had gross residual disease (R2), 63 (41.2%) had a positive margin of resection (R1), and 70 (45.8%) had complete resection with negative margins (R0). With a median follow-up of 63.9 months, 5-year, disease-specific survival, when stratified by R0/R1/R2 resection, was 94.4%, 87.6%, and 67.9%, respectively (P = .030). The data do not demonstrate a statistical difference in survival between R0 versus R1 (P = .222). The 5-year distant recurrence-free probability for M0 patients was 90.8%, 90.3%, and 70.7% (P = .410). The locoregional recurrence-free probability was 85.8% for R0 patients and 85.5% for R1 patients (P = .593).
Conclusion: With an appropriate operative strategy, patients with locally advanced thyroid cancer with an R0 or R1 resection have excellent survival outcome.
Copyright © 2016 Elsevier Inc. All rights reserved.
Figures
References
-
- Hay ID, Hutchinson ME, Gonzalez-Losada T, McIver B, Reinalda ME, Grant CS, et al. Papillary thyroid microcarcinoma: A study of 900 cases observed in a 60-year period. Surgery. 2008;144:980–7. discussion 987-8. - PubMed
-
- Shah JP, Loree TR, Dharker D, Strong EW, Begg C, Vlamis V. Prognostic factors in differentiated carcinoma of the thyroid gland. Am J Surg. 1992;164:658–61. - PubMed
-
- Hundahl SA, Cady B, Cunningham MP, Mazzaferri E, McKee RF, Rosai J, et al. Initial results from a prospective cohort study of 5583 cases of thyroid carcinoma treated in the United States during 1996. U.S. and German Thyroid Cancer Study Group An American College of Surgeons Commission on Cancer Patient Care Evaluation study. Cancer. 2000;89:202–17. - PubMed
-
- Hughes DT, Haymart MR, Miller BS, Gauger PG, Doherty GM. The most commonly occurring papillary thyroid cancer in the United States is now a microcarcinoma in a patient older than 45 years. Thyroid. 2011;21:231–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
