

Five-year histological and serological follow-up of operationally tolerant pediatric liver transplant recipients enrolled in WISP-R
- PMID: 27302659
- PMCID: PMC5159322
- DOI: 10.1002/hep.28681
Five-year histological and serological follow-up of operationally tolerant pediatric liver transplant recipients enrolled in WISP-R
Abstract
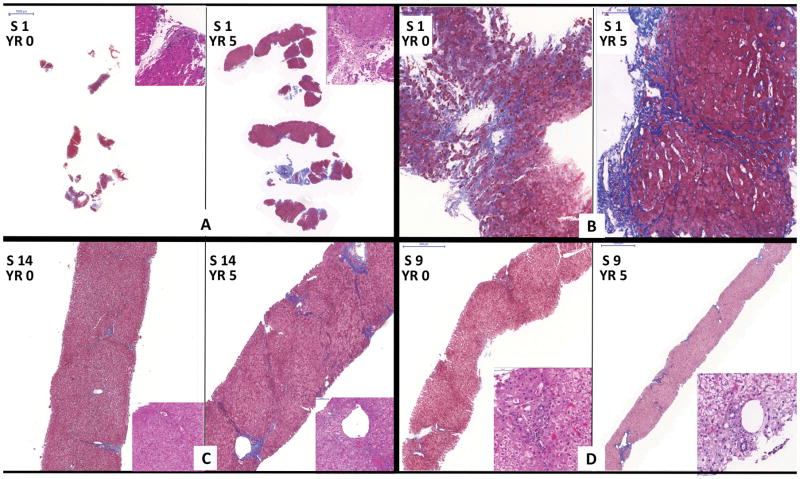
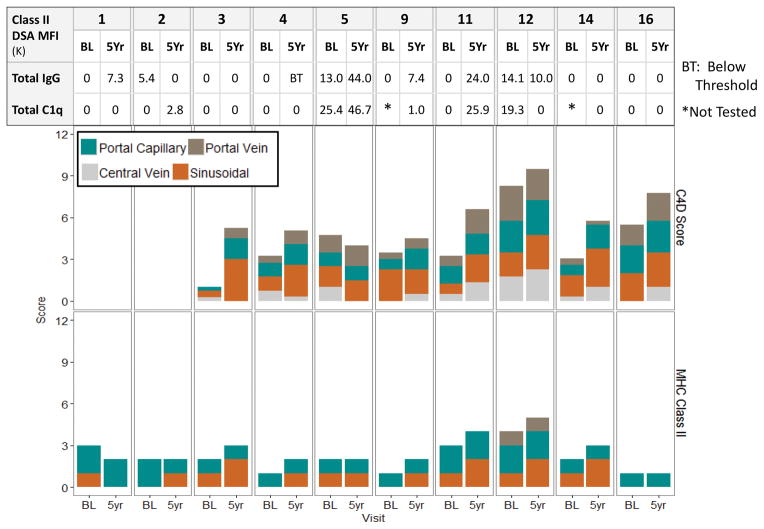
Pediatric liver transplant recipients arguably have the most to gain and the most to lose from discontinuing immunosuppression (IS). Whereas IS undoubtedly exerts a cumulative toll, there is concern that insufficient or no IS may contribute to allograft deterioration. Twelve pediatric recipients of parental living donor liver grafts, identified as operationally tolerant through complete IS withdrawal (WISP-R; NCT00320606), were followed for a total of 5 years (1 year of IS withdrawal and 4 years off IS) with serial liver tests and autoantibody and alloantibody assessments. Liver biopsies were performed 2 and 4 years off IS, and, at these time points, immunoglobulin G (IgG) subclass and C1q binding activity for donor-specific antibodies (DSAs) were determined. There were no cases of chronic rejection, graft loss, or death. Allografts did not exhibit progressive increase in inflammation or fibrosis. Smooth-muscle actin expression by stellate cells and CD34 expression by liver sinusoidal endothelial cells remained stable, consistent with the absence of progressive graft injury. Three subjects never exhibited DSA. However, 3 subjects showed intermittent de novo class I DSA, 4 subjects showed persistent de novo class II DSA, and 5 subjects showed persistent preexisting class II DSA. Class II DSA was predominantly against donor DQ antigens, often of high mean fluorescence intensity, rarely of the IgG3 subclass, and often capable of binding C1q.
Conclusion: Operationally tolerant pediatric liver transplant recipients maintain generally stable allograft histology in spite of apparently active humoral allo-immune responses. The absence of increased inflammation or progressive fibrosis suggests that a subset of liver allografts seem resistant to the chronic injury that is characteristic of antibody-mediated damage. (Hepatology 2017;65:647-660).
© 2016 by the American Association for the Study of Liver Diseases.
Figures






Comment in
-
Tolerance in clinical liver transplantation: The long road ahead.Hepatology. 2017 Feb;65(2):411-413. doi: 10.1002/hep.28862. Epub 2016 Nov 22. Hepatology. 2017. PMID: 27718261 No abstract available.
References
-
- Londono MC, Rimola A, O’Grady J, Sanchez-Fueyo A. Immunosuppression minimization vs. complete drug withdrawal in liver transplantation. J Hepatol. 2013;59:872–879. - PubMed
-
- Orlando G, Manzia T, Baiocchi L, Sanchez-Fueyo A, Angelico M, Tisone G. The Tor Vergata weaning off immunosuppression protocol in stable HCV liver transplant patients: the updated follow up at 78 months. Transpl Immunol. 2008;20:43–47. - PubMed
-
- Ekong UD, Melin-Aldana H, Seshadri R, Lokar J, Harris D, Whitington PF, Alonso EM. Graft histology characteristics in long-term survivors of pediatric liver transplantation. Liver Transpl. 2008;14:1582–1587. - PubMed
-
- Evans HM, Kelly DA, McKiernan PJ, Hubscher S. Progressive histological damage in liver allografts following pediatric liver transplantation. Hepatology. 2006;43:1109–1117. - PubMed
-
- Miyagawa-Hayashino A, Yoshizawa A, Uchida Y, Egawa H, Yurugi K, Masuda S, Minamiguchi S, et al. Progressive graft fibrosis and donor-specific human leukocyte antigen antibodies in pediatric late liver allografts. Liver Transpl. 2012;18:1333–1342. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
