

A 4-miRNA signature predicts the therapeutic outcome of glioblastoma
- PMID: 27302927
- PMCID: PMC5216759
- DOI: 10.18632/oncotarget.9945
A 4-miRNA signature predicts the therapeutic outcome of glioblastoma
Abstract
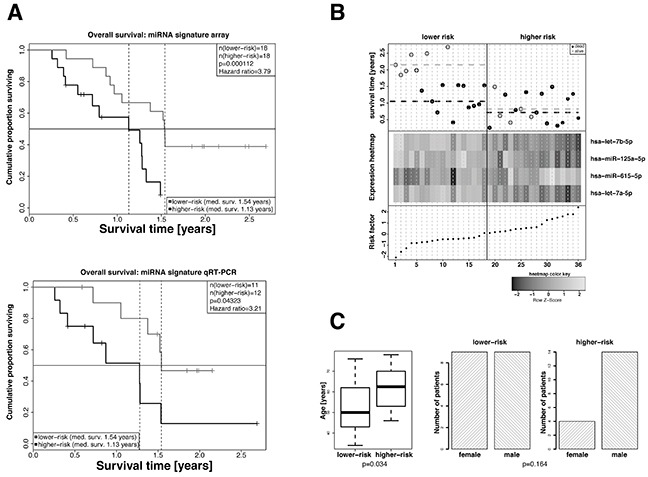
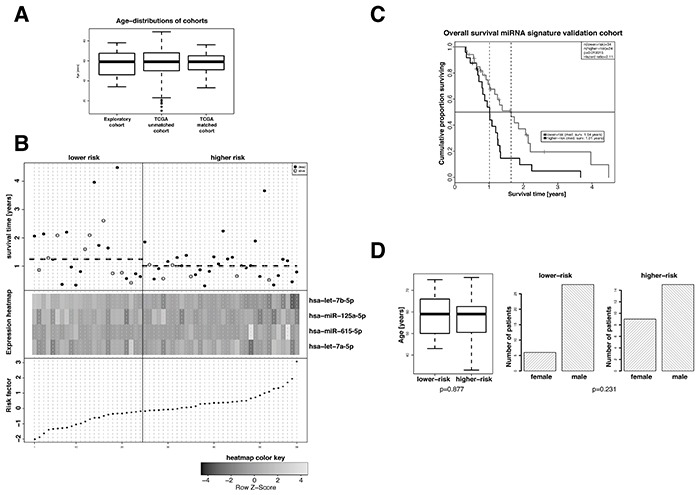
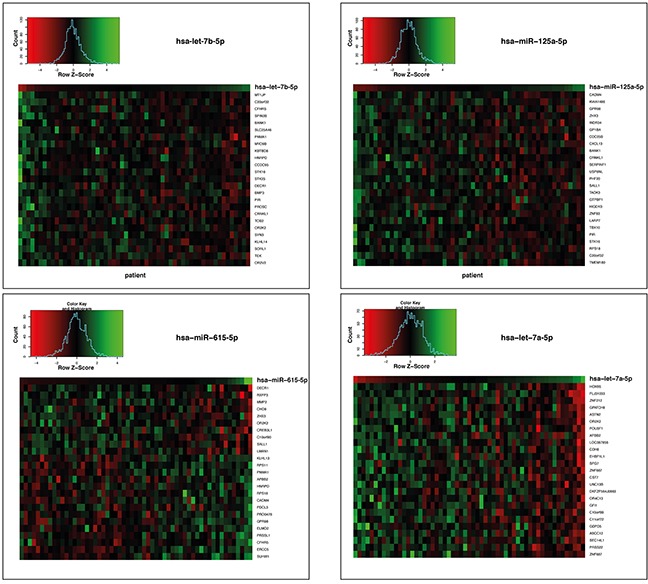
Multimodal therapy of glioblastoma (GBM) reveals inter-individual variability in terms of treatment outcome. Here, we examined whether a miRNA signature can be defined for the a priori identification of patients with particularly poor prognosis.FFPE sections from 36 GBM patients along with overall survival follow-up were collected retrospectively and subjected to miRNA signature identification from microarray data. A risk score based on the expression of the signature miRNAs and cox-proportional hazard coefficients was calculated for each patient followed by validation in a matched GBM subset of TCGA. Genes potentially regulated by the signature miRNAs were identified by a correlation approach followed by pathway analysis.A prognostic 4-miRNA signature, independent of MGMT promoter methylation, age, and sex, was identified and a risk score was assigned to each patient that allowed defining two groups significantly differing in prognosis (p-value: 0.0001, median survival: 10.6 months and 15.1 months, hazard ratio = 3.8). The signature was technically validated by qRT-PCR and independently validated in an age- and sex-matched subset of standard-of-care treated patients of the TCGA GBM cohort (n=58). Pathway analysis suggested tumorigenesis-associated processes such as immune response, extracellular matrix organization, axon guidance, signalling by NGF, GPCR and Wnt. Here, we describe the identification and independent validation of a 4-miRNA signature that allows stratification of GBM patients into different prognostic groups in combination with one defined threshold and set of coefficients that could be utilized as diagnostic tool to identify GBM patients for improved and/or alternative treatment approaches.
Keywords: glioblastoma; miRNA; signature.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Fisher JL, Schwartzbaum JA, Wrensch M, Wiemels JL. Epidemiology of brain tumors. Neurol Clin. 2007;25:867–890. vii. - PubMed
-
- Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJ, Janzer RC, Ludwin SK, Allgeier A, Fisher B, Belanger K, Hau P, Brandes AA, Gijtenbeek J, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009;10:459–466. - PubMed
-
- Chinot OL, de La Motte Rouge T, Moore N, Zeaiter A, Das A, Phillips H, Modrusan Z, Cloughesy T. AVAglio: Phase 3 trial of bevacizumab plus temozolomide and radiotherapy in newly diagnosed glioblastoma multiforme. Adv Ther. 2011;28:334–340. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
