

Current status of laparoscopic liver resection for hepatocellular carcinoma
- PMID: 27304550
- PMCID: PMC4946407
- DOI: 10.3350/cmh.2016.0026
Current status of laparoscopic liver resection for hepatocellular carcinoma
Abstract
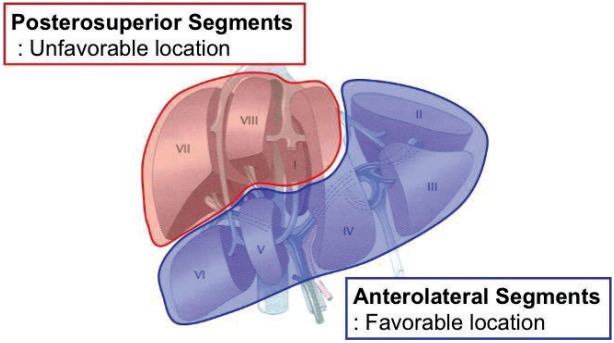
Laparoscopic liver resection (LLR) is becoming widely accepted for the treatment of hepatocellular carcinoma (HCC). Laparoscopic left lateral sectionectomy and minor laparoscopic liver resection are now considered standard approaches, especially for tumors located in the anterolateral segments of the liver. Laparoscopic left lateral sectionectomy in adult donors is also gaining acceptance for child liver transplantation in many centers. Major LLRs, including left hepatectomy and right hepatectomy, have been recently attempted. Laparoscopic donor hepatectomy is becoming more popular owing to increasing demand from young living donors who appreciate its minimal invasiveness and excellent cosmetic outcomes. Several centers have performed total laparoscopic donor right hepatectomy in adult-to-adult living donor liver transplantation. Many meta-analyses have shown that LLR is better than open liver resection in terms of short-term outcomes, principally cosmetic outcomes. Although no randomized control trials have compared LLR with open liver resection, the long-term oncologic outcomes were similar for both procedures in recent case-matched studies.
Keywords: Hepatectomy; Laparoscopy; Outcome; Prognosis; Recurrence.
Conflict of interest statement
Figures
References
-
- El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology. 2007;132:2557–2576. - PubMed
-
- Llovet JM, Bruix J. Novel advancements in the management of hepatocellular carcinoma in 2008. J Hepatol. 2008;48(Suppl 1):S20–S37. - PubMed
-
- Jaskille A, Schechner A, Park K, Williams M, Wang D, Sava J. Abdominal insufflation decreases blood loss and mortality after porcine liver injury. J Trauma. 2005;59:1305–1308. discussion 1308. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
