

Patients with Tuberculosis Have a Dysfunctional Circulating B-Cell Compartment, Which Normalizes following Successful Treatment
- PMID: 27304615
- PMCID: PMC4909319
- DOI: 10.1371/journal.ppat.1005687
Patients with Tuberculosis Have a Dysfunctional Circulating B-Cell Compartment, Which Normalizes following Successful Treatment
Abstract
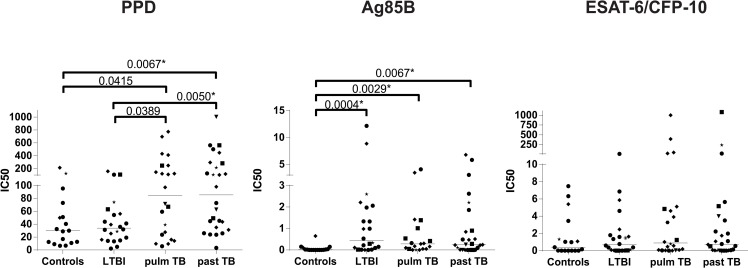
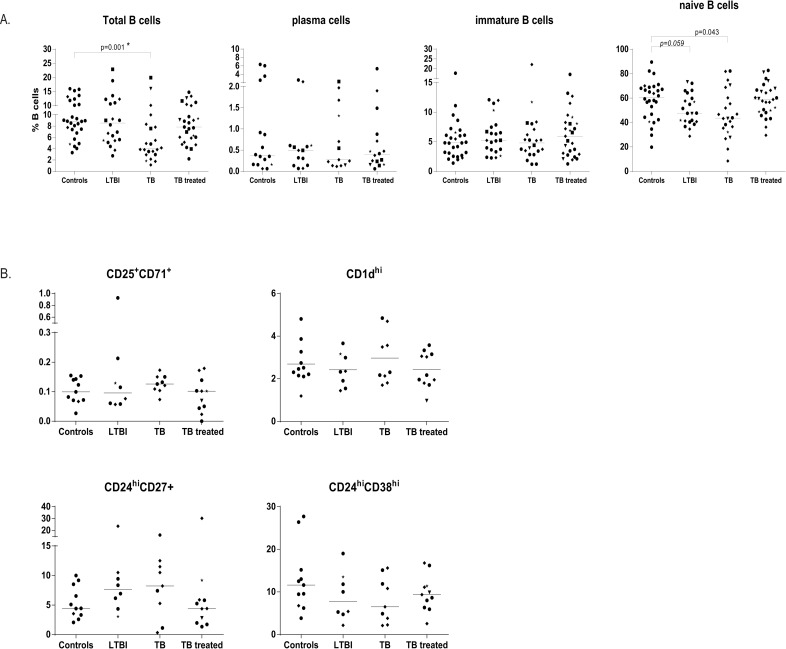
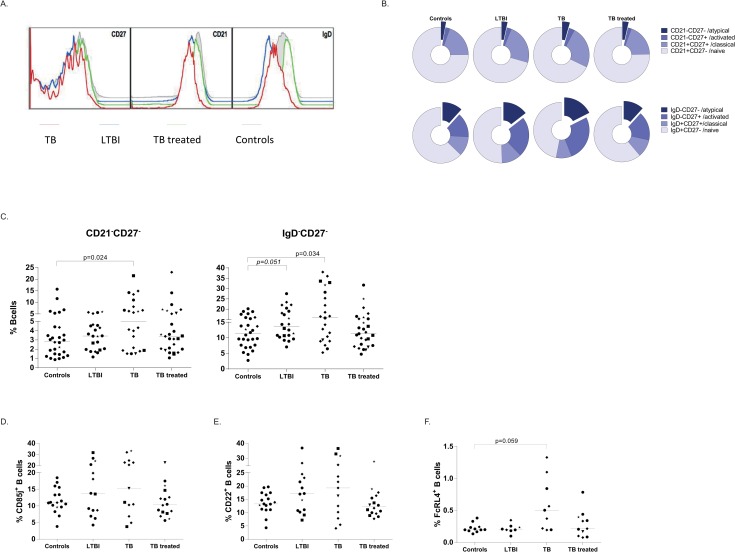
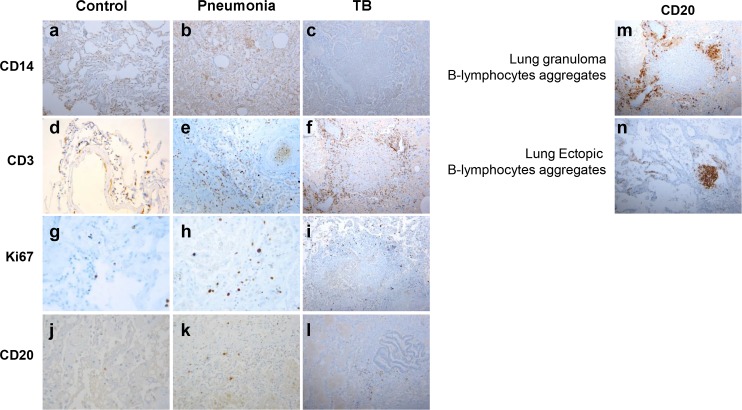
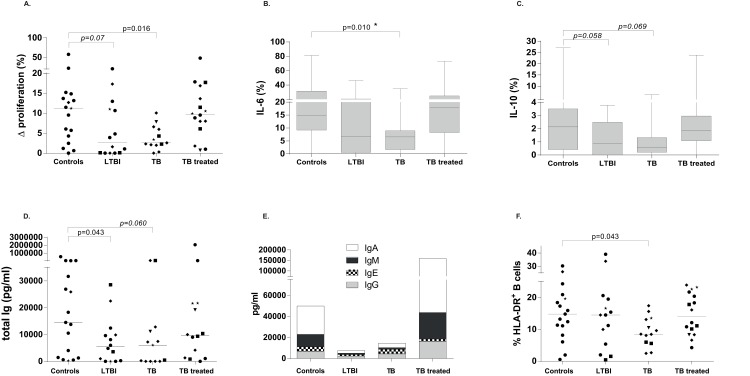
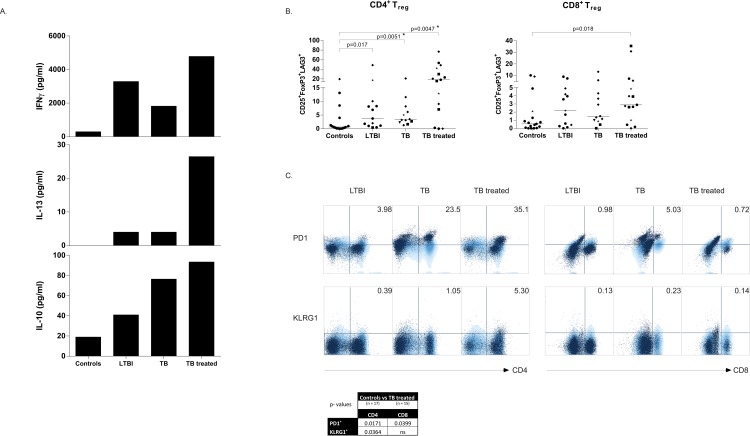
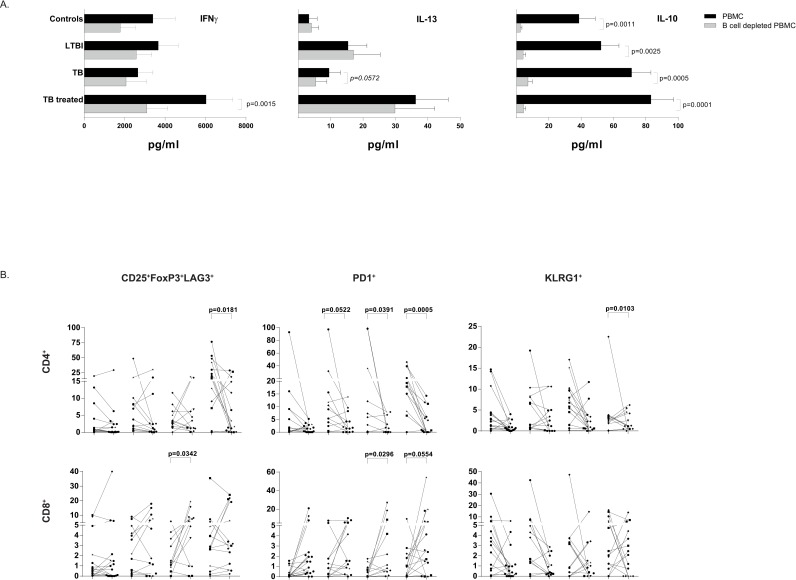
B-cells not only produce immunoglobulins and present antigens to T-cells, but also additional key roles in the immune system. Current knowledge on the role of B-cells in infections caused by intracellular bacteria is fragmentary and contradictory. We therefore analysed the phenotypical and functional properties of B-cells during infection and disease caused by Mycobacterium tuberculosis (Mtb), the bacillus causing tuberculosis (TB), and included individuals with latent TB infection (LTBI), active TB, individuals treated successfully for TB, and healthy controls. Patients with active or treated TB disease had an increased proportion of antibodies reactive with mycobacteria. Patients with active TB had reduced circulating B-cell frequencies, whereas only minor increases in B-cells were detected in the lungs of individuals deceased from TB. Both active TB patients and individuals with LTBI had increased relative fractions of B-cells with an atypical phenotype. Importantly, these B-cells displayed impaired proliferation, immunoglobulin- and cytokine- production. These defects disappeared upon successful treatment. Moreover, T-cell activity was strongest in individuals successfully treated for TB, compared to active TB patients and LTBI subjects, and was dependent on the presence of functionally competent B-cells as shown by cellular depletion experiments. Thus, our results reveal that general B-cell function is impaired during active TB and LTBI, and that this B-cell dysfunction compromises cellular host immunity during Mtb infection. These new insights may provide novel strategies for correcting Mtb infection-induced immune dysfunction towards restored protective immunity.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Lombardi G, del GF, Vismara D, Piccolella E, de Martino C, Garzelli C et al. Epstein-Barr virus-transformed B cells process and present Mycobacterium tuberculosis particulate antigens to T-cell clones. Cell Immunol. 1987; 107: 281–292. - PubMed
-
- Garcia-Perez BE, De la Cruz-Lopez JJ, Castaneda-Sanchez JI, Munoz-Duarte AR, Hernandez-Perez AD, Villegas-Castrejon H et al. Macropinocytosis is responsible for the uptake of pathogenic and non-pathogenic mycobacteria by B lymphocytes (Raji cells). BMC Microbiol. 2012; 12: 246 10.1186/1471-2180-12-246 - DOI - PMC - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
