

Estimation of Benefits, Burden, and Harms of Colorectal Cancer Screening Strategies: Modeling Study for the US Preventive Services Task Force
- PMID: 27305518
- PMCID: PMC5493310
- DOI: 10.1001/jama.2016.6828
Estimation of Benefits, Burden, and Harms of Colorectal Cancer Screening Strategies: Modeling Study for the US Preventive Services Task Force
Abstract
Importance: The US Preventive Services Task Force (USPSTF) is updating its 2008 colorectal cancer (CRC) screening recommendations.
Objective: To inform the USPSTF by modeling the benefits, burden, and harms of CRC screening strategies; estimating the optimal ages to begin and end screening; and identifying a set of model-recommendable strategies that provide similar life-years gained (LYG) and a comparable balance between LYG and screening burden.
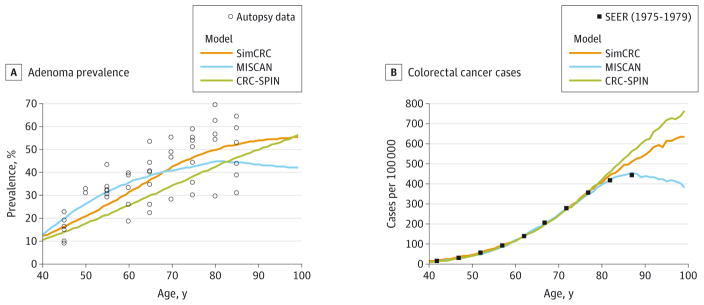
Design, setting, and participants: Comparative modeling with 3 microsimulation models of a hypothetical cohort of previously unscreened US 40-year-olds with no prior CRC diagnosis.
Exposures: Screening with sensitive guaiac-based fecal occult blood testing, fecal immunochemical testing (FIT), multitarget stool DNA testing, flexible sigmoidoscopy with or without stool testing, computed tomographic colonography (CTC), or colonoscopy starting at age 45, 50, or 55 years and ending at age 75, 80, or 85 years. Screening intervals varied by modality. Full adherence for all strategies was assumed.
Main outcomes and measures: Life-years gained compared with no screening (benefit), lifetime number of colonoscopies required (burden), lifetime number of colonoscopy complications (harms), and ratios of incremental burden and benefit (efficiency ratios) per 1000 40-year-olds.
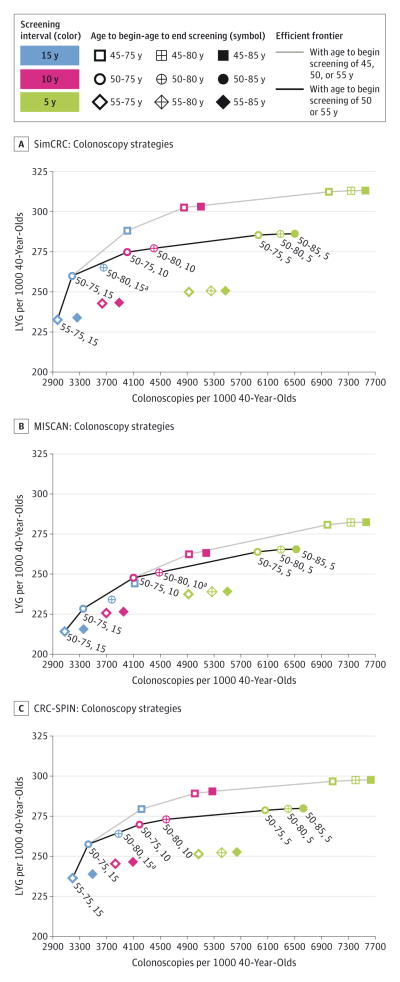
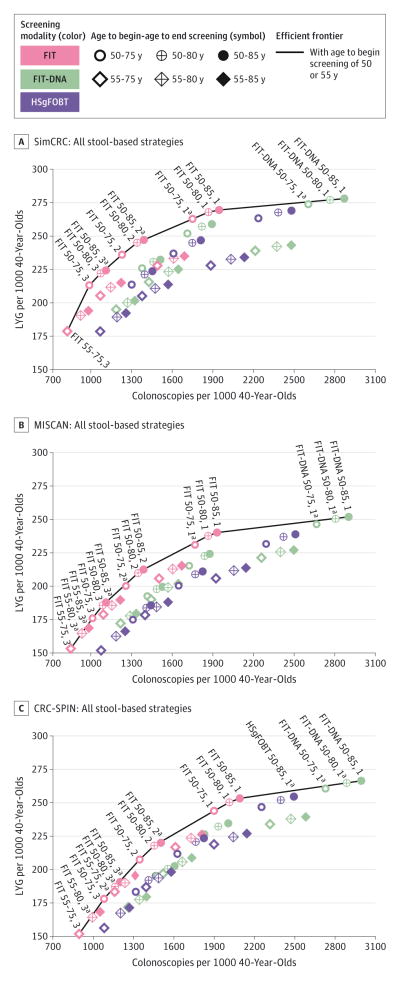
Results: The screening strategies provided LYG in the range of 152 to 313 per 1000 40-year-olds. Lifetime colonoscopy burden per 1000 persons ranged from fewer than 900 (FIT every 3 years from ages 55-75 years) to more than 7500 (colonoscopy screening every 5 years from ages 45-85 years). Harm from screening was at most 23 complications per 1000 persons screened. Strategies with screening beginning at age 50 years generally provided more LYG as well as more additional LYG per additional colonoscopy than strategies with screening beginning at age 55 years. There were limited empirical data to support a start age of 45 years. For persons adequately screened up to age 75 years, additional screening yielded small increases in LYG relative to the increase in colonoscopy burden. With screening from ages 50 to 75 years, 4 strategies yielded a comparable balance of screening burden and similar LYG (median LYG per 1000 across the models): colonoscopy every 10 years (270 LYG); sigmoidoscopy every 10 years with annual FIT (256 LYG); CTC every 5 years (248 LYG); and annual FIT (244 LYG).
Conclusions and relevance: In this microsimulation modeling study of a previously unscreened population undergoing CRC screening that assumed 100% adherence, the strategies of colonoscopy every 10 years, annual FIT, sigmoidoscopy every 10 years with annual FIT, and CTC every 5 years performed from ages 50 through 75 years provided similar LYG and a comparable balance of benefit and screening burden.
Conflict of interest statement
Figures

Comment in
-
In simulation modelling, there are multiple ways to effectively screen for colorectal cancer.Evid Based Med. 2017 Apr;22(2):59. doi: 10.1136/ebmed-2016-110521. Epub 2017 Jan 10. Evid Based Med. 2017. PMID: 28073866 No abstract available.
-
What is the optimal colorectal cancer screening program for an average-risk population?Transl Gastroenterol Hepatol. 2017 Mar 16;2:17. doi: 10.21037/tgh.2017.03.05. eCollection 2017. Transl Gastroenterol Hepatol. 2017. PMID: 28447052 Free PMC article. No abstract available.
References
-
- Mandel JS, Bond JH, Church TR, et al. Reducing mortality from colorectal cancer by screening for fecal occult blood: Minnesota Colon Cancer Control Study. N Engl J Med. 1993;328(19):1365–1371. - PubMed
-
- Hardcastle JD, Chamberlain JO, Robinson MH, et al. Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet. 1996;348(9040):1472–1477. - PubMed
-
- Kronborg O, Fenger C, Olsen J, Jorgensen OD, Sondergaard O. Randomised study of screening for colorectal cancer with faecal-occult-blood test. Lancet. 1996;348(9040):1467–1471. - PubMed
-
- Shaukat A, Mongin SJ, Geisser MS, et al. Long-term mortality after screening for colorectal cancer. N Engl J Med. 2013;369(12):1106–1114. - PubMed
-
- Atkin WS, Edwards R, Kralj-Hans I, et al. UK Flexible Sigmoidoscopy Trial Investigators. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet. 2010;375(9726):1624–1633. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
