

Patients with Obstructive Sleep Apnea Have Cardiac Repolarization Disturbances when Travelling to Altitude: Randomized, Placebo-Controlled Trial of Acetazolamide
- PMID: 27306264
- PMCID: PMC4989251
- DOI: 10.5665/sleep.6080
Patients with Obstructive Sleep Apnea Have Cardiac Repolarization Disturbances when Travelling to Altitude: Randomized, Placebo-Controlled Trial of Acetazolamide
Abstract
Study objectives: Obstructive sleep apnea (OSA) promotes myocardial electrical instability and may predispose to nocturnal sudden cardiac death. We evaluated whether hypobaric hypoxia during altitude travel further impairs cardiac repolarization in patients with OSA, and whether this is prevented by acetazolamide, a drug known to improve oxygenation and central sleep apnea at altitude.
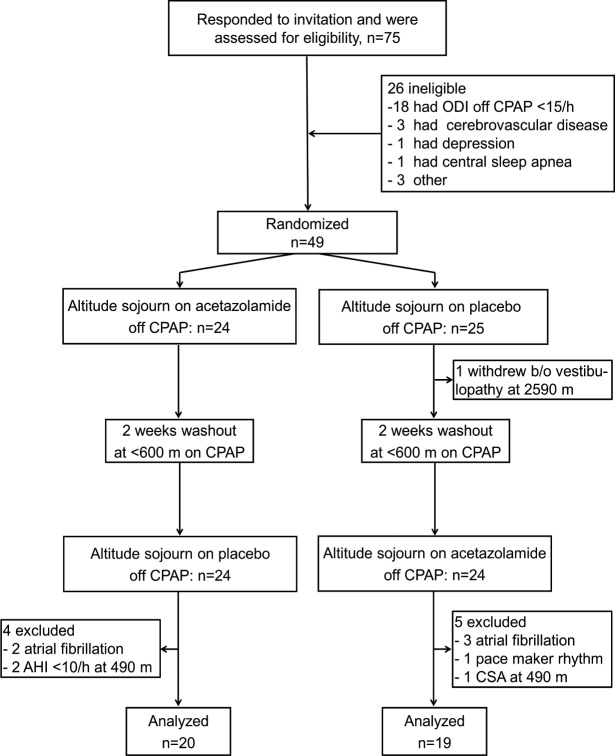
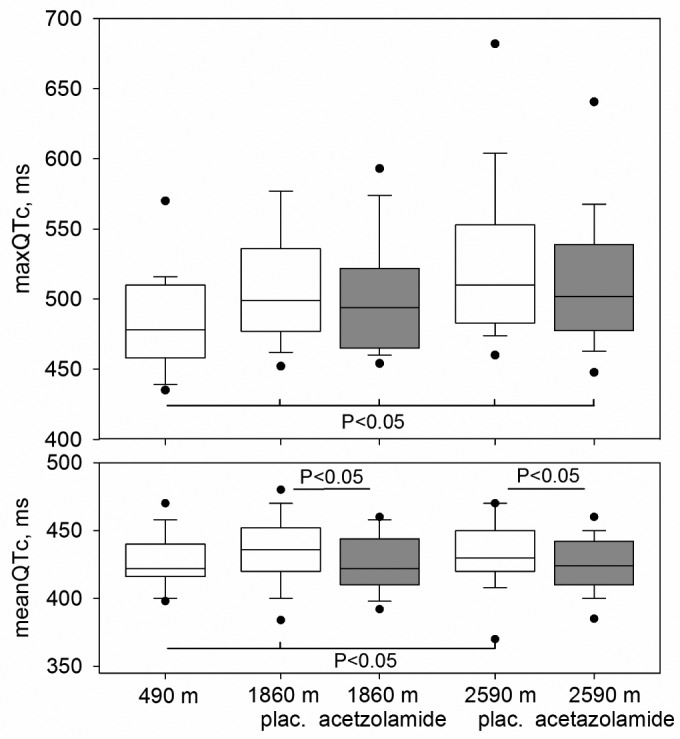
Methods: Thirty-nine OSA patients living < 600 m, discontinued continuous positive airway pressure therapy during studies at 490 m and during two sojourns of 3 days at altitude (2 days at 1860 m, 1 day at 2590 m). During one altitude sojourn, patients took acetazolamide, during the other placebo, or vice versa, according to a randomized, double-blind crossover design. Twelve-lead electrocardiography and pulse oximetry (SpO2) were recorded during nocturnal polysomnography. Heart rate corrected mean QT intervals during the entire night (meanQTc) and during 1 min of the night with the longest meanQTc (maxQTc) were determined.
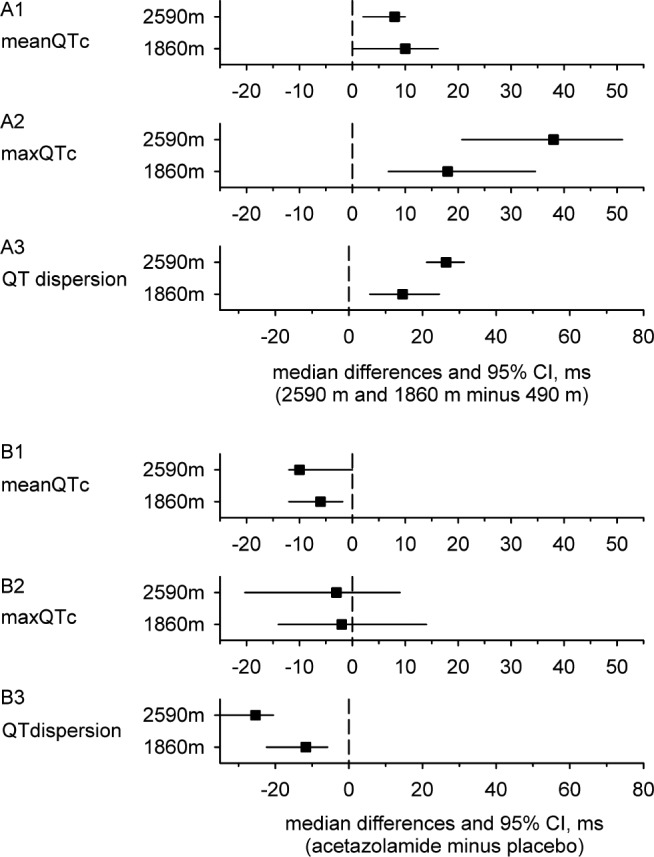
Results: At 490 m the median nocturnal SpO2 was 93%, medians of meanQTc and maxQTc were 420 ms and 478 ms. At 2590 m, on placebo, SpO2 was lower (85%), and meanQTc and maxQTc were prolonged to 430 ms and 510 ms (P < 0.02 vs. 490 m, all corresponding comparisons). At 2590 m on acetazolamide, median SpO2 was increased to 88% (P < 0.05 vs. placebo), meanQTc was reduced to 427 ms (P < 0.05 vs. placebo), whereas maxQTc remained increased at 502 ms (P = ns vs. placebo).
Conclusions: At 2590 m OSA patients experienced cardiac repolarization disturbances in association with hypoxemia. Prolongation of meanQTc at altitude was prevented and hypoxemia was improved by acetazolamide, whereas maxQTc remained increased suggesting imperfect protection from repolarization disturbances.
Clinical trial registration: ClinicalTrials.gov ID: NTC-00714740. URL: www.clinicaltrials.gov.
Keywords: altitude; cardiac arrhythmias; cardiac repolarization; sleep apnea; sudden cardiac death.
© 2016 Associated Professional Sleep Societies, LLC.
Figures
References
-
- Marin JM, Carrizo SJ, Vicente E, Agusti AG. Long-term cardiovascular outcomes in men with obstructive sleep apnoeahypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005;365:1046–53. - PubMed
-
- Kohler M, Stradling JR. Mechanisms of vascular damage in obstructive sleep apnea. Nature reviews. Cardiology. 2010;7:677–85. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
