

Polypharmacy and effects of apixaban versus warfarin in patients with atrial fibrillation: post hoc analysis of the ARISTOTLE trial
- PMID: 27306620
- PMCID: PMC4908974
- DOI: 10.1136/bmj.i2868
Polypharmacy and effects of apixaban versus warfarin in patients with atrial fibrillation: post hoc analysis of the ARISTOTLE trial
Abstract
Objective: To determine whether the treatment effect of apixaban versus warfarin differs with increasing numbers of concomitant drugs used by patients with atrial fibrillation.
Design: Post hoc analysis performed in 2015 of results from ARISTOTLE (apixaban for reduction in stroke and other thromboembolic events in atrial fibrillation)-a multicentre, double blind, double dummy trial that started in 2006 and ended in 2011.
Participants: 18 201 ARISTOTLE trial participants.
Interventions: In the ARISTOTLE trial, patients were randomised to either 5 mg apixaban twice daily (n=9120) or warfarin (target international normalised ratio range 2.0-3.0; n=9081). In the post hoc analysis, patients were divided into groups according to the number of concomitant drug treatments used at baseline (0-5, 6-8, ≥9 drugs) with a median follow-up of 1.8 years.
Main outcome measures: Clinical outcomes and treatment effects of apixaban versus warfarin (adjusted for age, sex, and country).
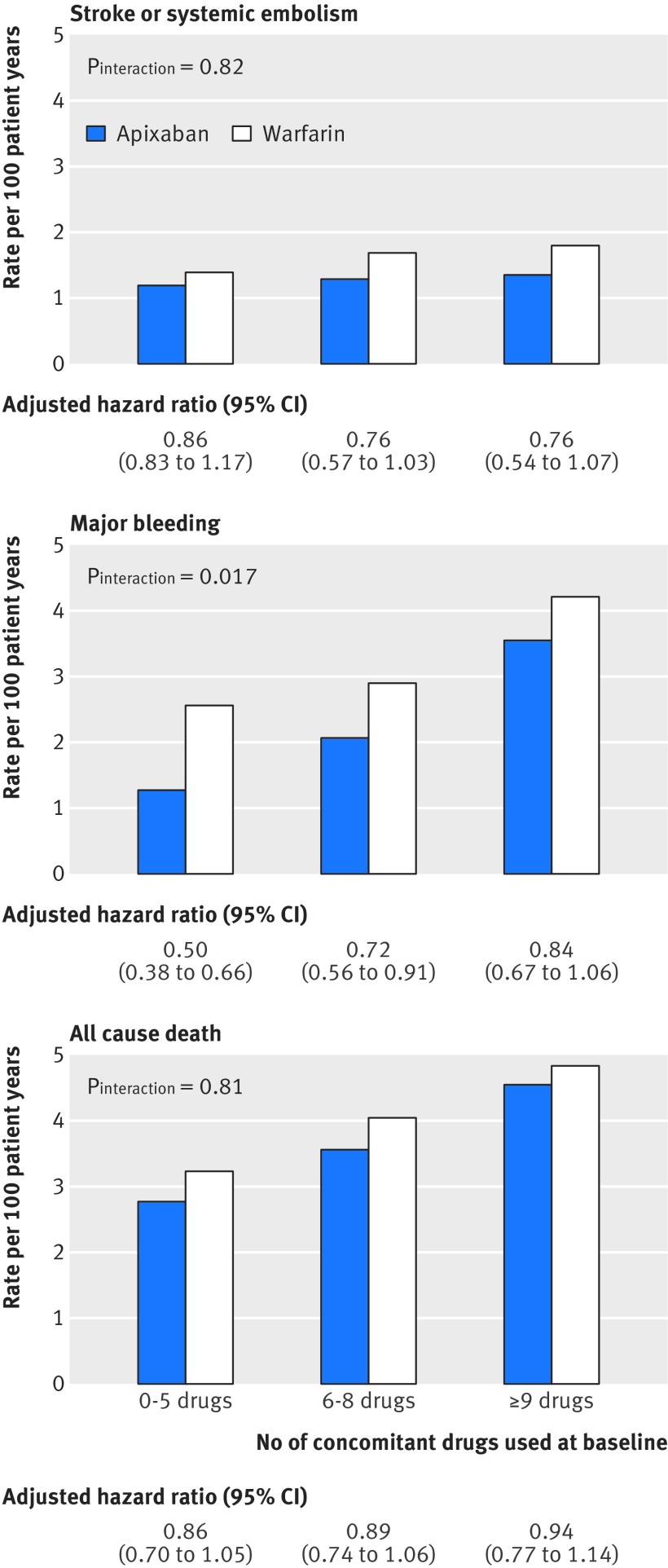
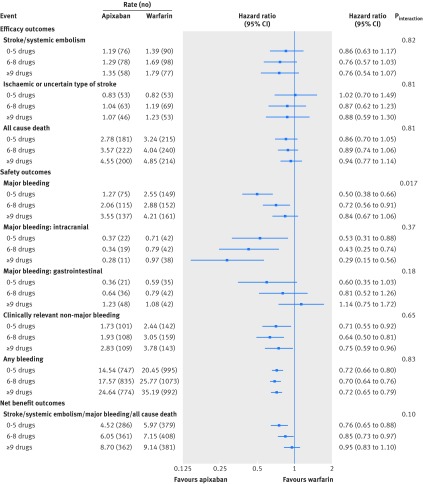
Results: Each patient used a median of six drugs (interquartile range 5-9); polypharmacy (≥5 drugs) was seen in 13 932 (76.5%) patients. Greater numbers of concomitant drugs were used in older patients, women, and patients in the United States. The number of comorbidities increased across groups of increasing numbers of drugs (0-5, 6-8, ≥9 drugs), as did the proportions of patients treated with drugs that interact with warfarin or apixaban. Mortality also rose significantly with the number of drug treatments (P<0.001), as did rates of stroke or systemic embolism (1.29, 1.48, and 1.57 per 100 patient years, for 0-5, 6-8, and ≥9 drugs, respectively) and major bleeding (1.91, 2.46, and 3.88 per 100 patient years, respectively). Relative risk reductions in stroke or systemic embolism for apixaban versus warfarin were consistent, regardless of the number of concomitant drugs (Pinteraction=0.82). A smaller reduction in major bleeding was seen with apixaban versus warfarin with increasing numbers of concomitant drugs (Pinteraction=0.017). Patients with interacting (potentiating) drugs for warfarin or apixaban had similar outcomes and consistent treatment effects of apixaban versus warfarin.
Conclusions: In the ARISTOTLE trial, three quarters of patients had polypharmacy; this subgroup had an increased comorbidity, more interacting drugs, increased mortality, and higher rates of thromboembolic and bleeding complications. In terms of a potential differential response to anticoagulation therapy in patients with atrial fibrillation and polypharmacy, apixaban was more effective than warfarin, and is at least just as safe.Trial registration ARISTOTLE trial, ClinicalTrials.gov NCT00412984.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
References
-
- GBD 2013 Mortality and Causes of Death Collaborators. Global, regional, and national age-sex specific all-cause and cause-specific mortality for 240 causes of death, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet 2015;385:117-71. 10.1016/S0140-6736(14)61682-2 pmid:25530442. - DOI - PMC - PubMed
-
- Nieuwlaat R, Olsson SB, Lip GYH, et al. Euro Heart Survey Investigators Euro Heart Survey on Atrial Fibrillation. Guideline-adherent antithrombotic treatment is associated with improved outcomes compared with undertreatment in high-risk patients with atrial fibrillation. Am Heart J 2007;153:1006-12. 10.1016/j.ahj.2007.03.008 pmid:17540203. - DOI - PubMed
-
- Scowcroft AC, Lee S, Mant J. Thromboprophylaxis of elderly patients with AF in the UK: an analysis using the General Practice Research Database (GPRD) 2000-2009. Heart 2013;99:127-32. 10.1136/heartjnl-2012-302843 pmid:23086966. - DOI - PMC - PubMed
-
- Singh S, Bajorek B. Pharmacotherapy in the ageing patient: the impact of age per se (a review). Ageing Res Rev 2015;24:99-110. 10.1016/j.arr.2015.07.006 pmid:26226330. - DOI - PubMed
-
- Jyrkkä J, Enlund H, Korhonen MJ, Sulkava R, Hartikainen S. Patterns of drug use and factors associated with polypharmacy and excessive polypharmacy in elderly persons: results of the Kuopio 75+ study: a cross-sectional analysis. Drugs Aging 2009;26:493-503. 10.2165/00002512-200926060-00006 pmid:19591524. - DOI - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical