

Antibiotics, birth mode, and diet shape microbiome maturation during early life
- PMID: 27306664
- PMCID: PMC5308924
- DOI: 10.1126/scitranslmed.aad7121
Antibiotics, birth mode, and diet shape microbiome maturation during early life
Abstract
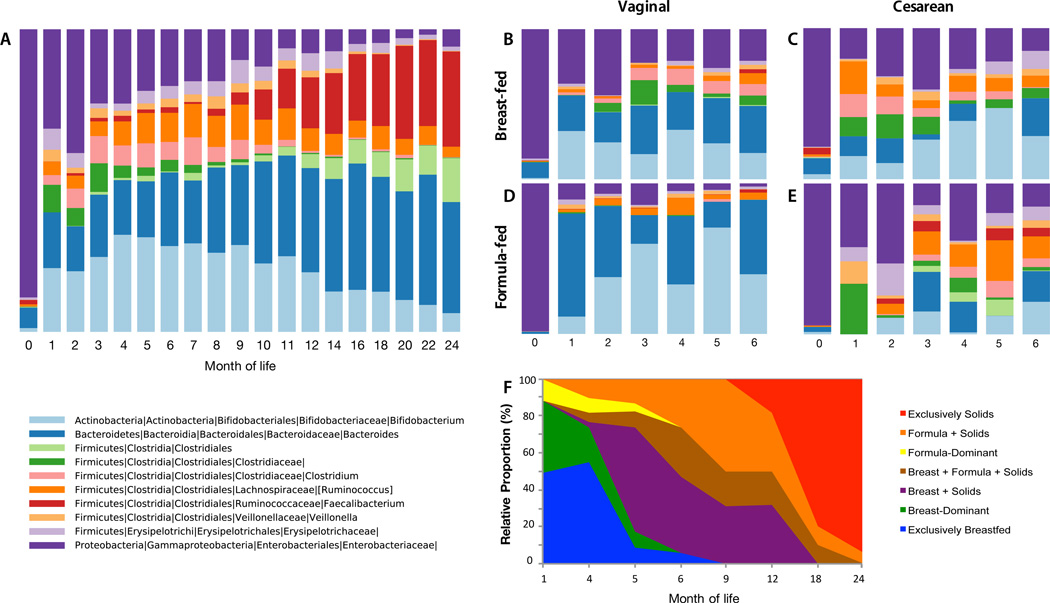
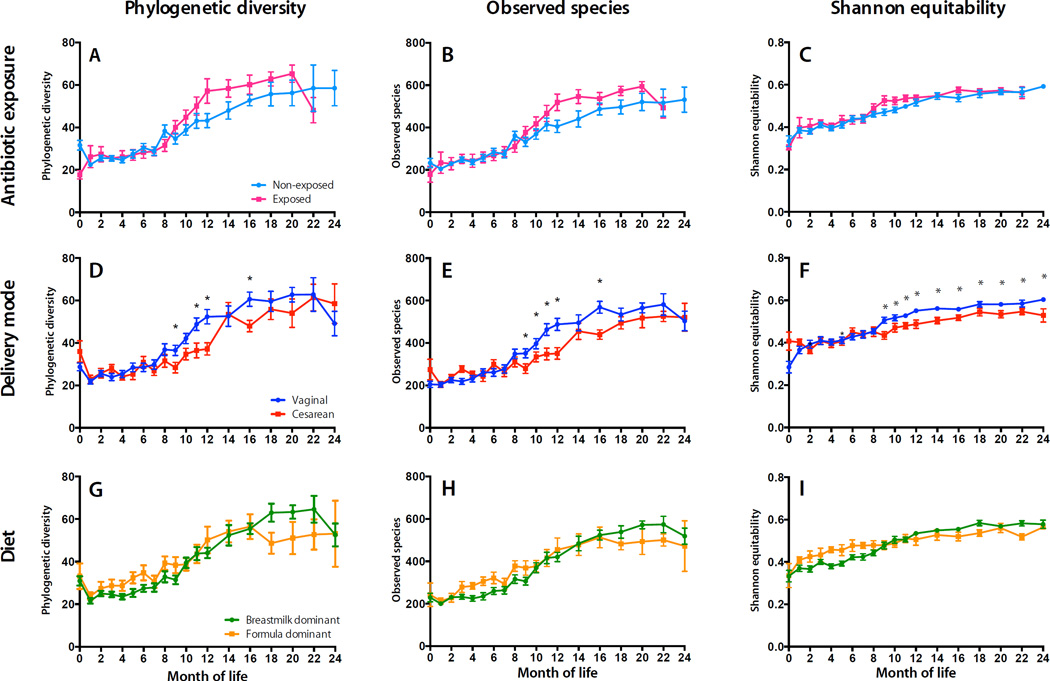
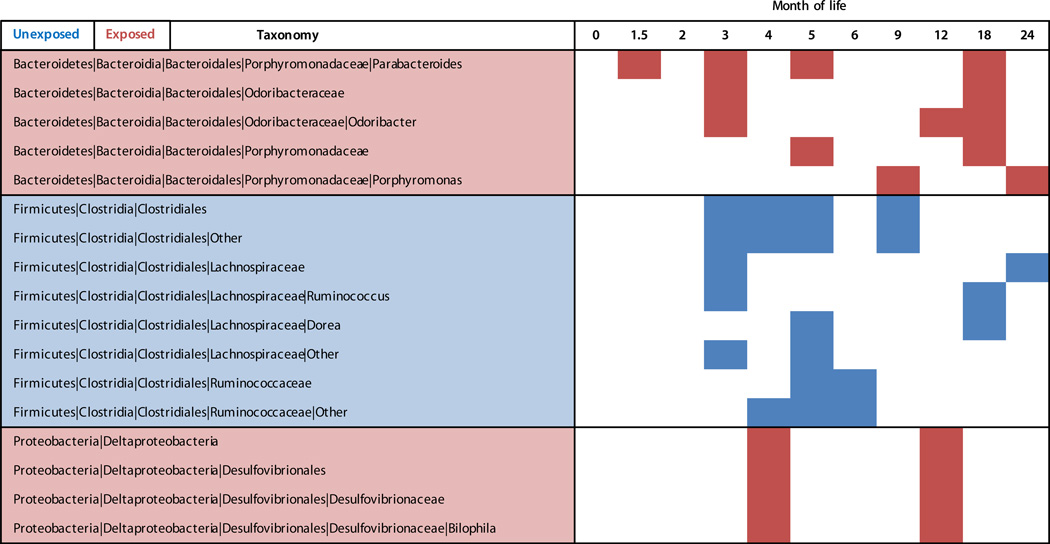
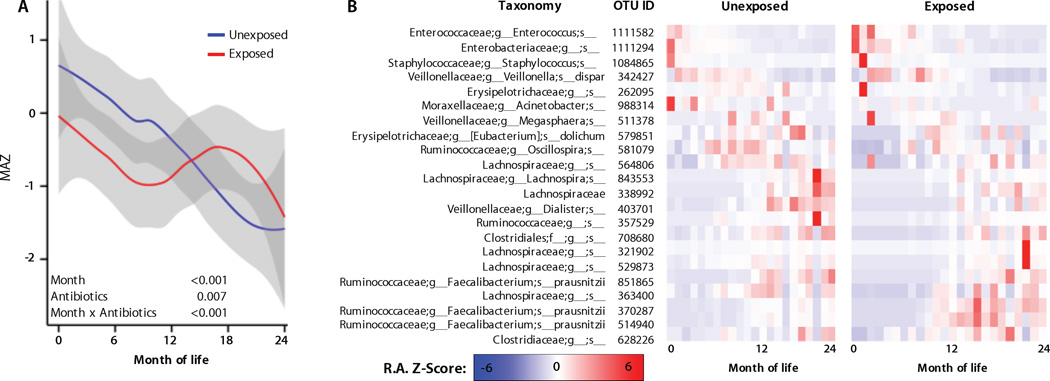
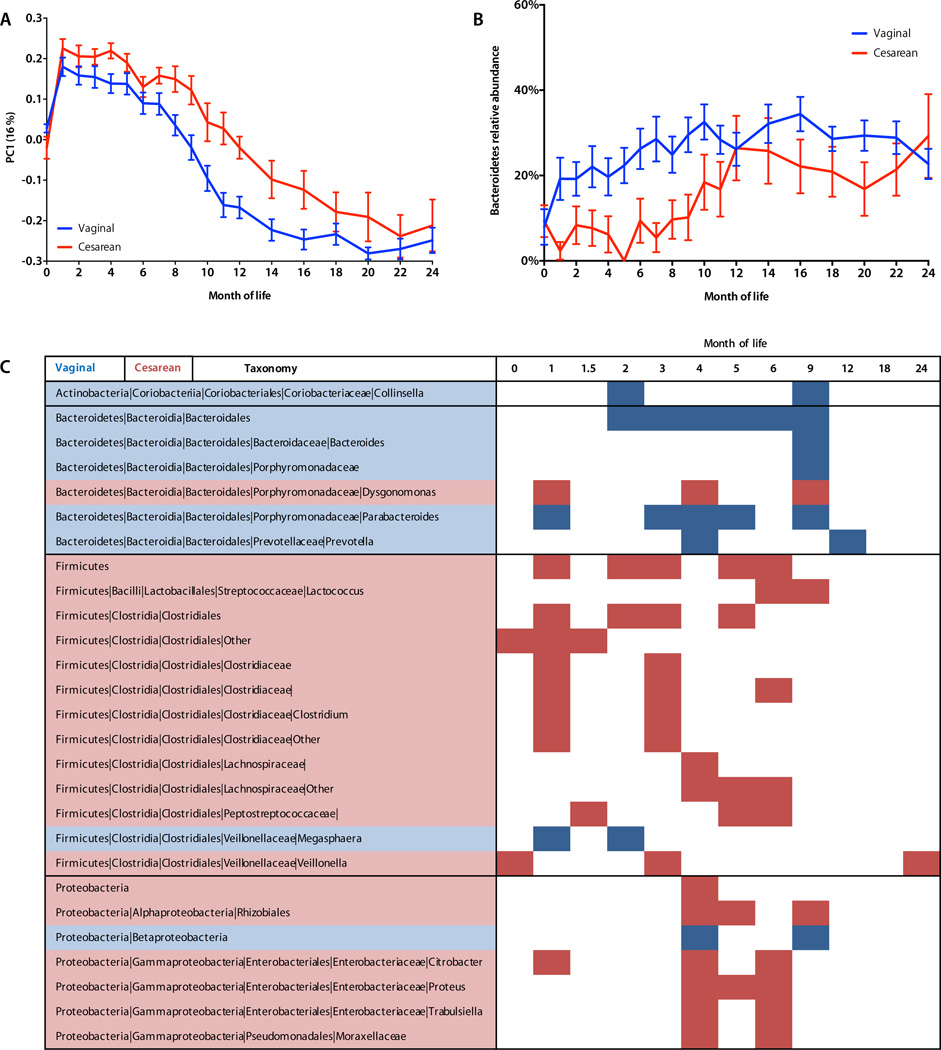
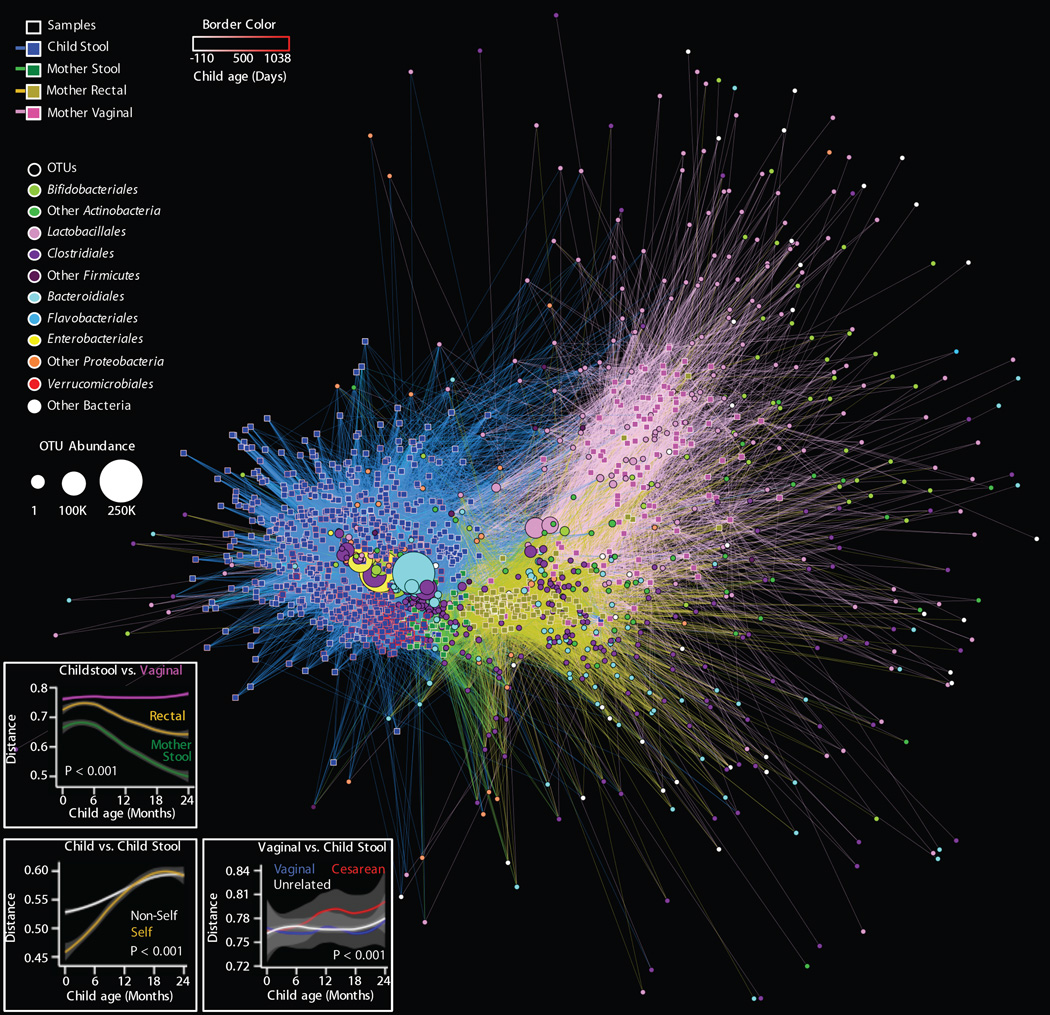
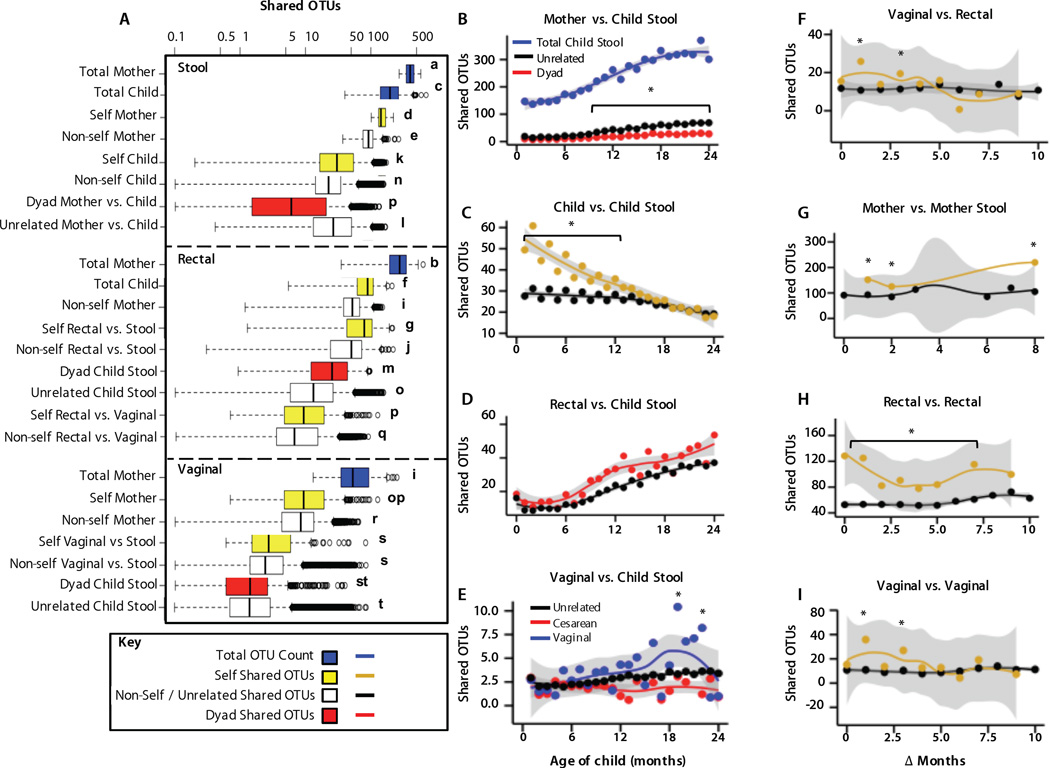
Early childhood is a critical stage for the foundation and development of both the microbiome and host. Early-life antibiotic exposures, cesarean section, and formula feeding could disrupt microbiome establishment and adversely affect health later in life. We profiled microbial development during the first 2 years of life in a cohort of 43 U.S. infants and identified multiple disturbances associated with antibiotic exposures, cesarean section, and formula feeding. These exposures contributed to altered establishment of maternal bacteria, delayed microbiome development, and altered α-diversity. These findings illustrate the complexity of early-life microbiome development and its sensitivity to perturbation.
Copyright © 2016, American Association for the Advancement of Science.
Figures
Comment in
-
Gut microbiota: First steps in the infant gut microbiota.Nat Rev Gastroenterol Hepatol. 2016 Aug;13(8):437. doi: 10.1038/nrgastro.2016.108. Epub 2016 Jul 6. Nat Rev Gastroenterol Hepatol. 2016. PMID: 27381073 No abstract available.
References
-
- Renz H, Brandtzaeg P, Hornef M. The impact of perinatal immune development on mucosal homeostasis and chronic inflammation. Nature Reviews Immunology. 2012;12:9–23. - PubMed
-
- Turnbaugh PJ, Ley RE, Mahowald MA, Magrini V, Mardis ER, Gordon JI. An obesity-associated gut microbiome with increased capacity for energy harvest. Nature. 2006;444:1027–1031. - PubMed
-
- Subramanian S, Huq S, Yatsunenko T, Haque R, Mahfuz M, Alam MA, Benezra A, DeStefano J, Meier MF, Muegge BD, Barratt MJ, VanArendonk LG, Zhang Q, Province MA, Petri WA, Jr, Ahmed T, Gordon JI. Persistent gut microbiota immaturity in malnourished Bangladeshi children. Nature. 2014;510:417–421. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
