

Inflammatory arthritis and sicca syndrome induced by nivolumab and ipilimumab
- PMID: 27307501
- PMCID: PMC5333990
- DOI: 10.1136/annrheumdis-2016-209595
Inflammatory arthritis and sicca syndrome induced by nivolumab and ipilimumab
Abstract
Objectives: Immune checkpoint inhibitors (ICIs) targeting the cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and programmed cell death protein 1 (PD-1) pathways have demonstrated survival improvements in multiple advanced cancers, but also cause immune-related adverse events (IRAEs). IRAEs with clinical features similar to rheumatic diseases have not been well described. We report patients with inflammatory arthritis and sicca syndrome secondary to ICIs.
Methods: We report patients evaluated in the Johns Hopkins Rheumatology clinics from 2012 to 2016 identified as having new rheumatological symptoms in the context of treatment with ipilimumab (anti-CTLA-4) and/or nivolumab (anti-PD-1) for solid tumours.
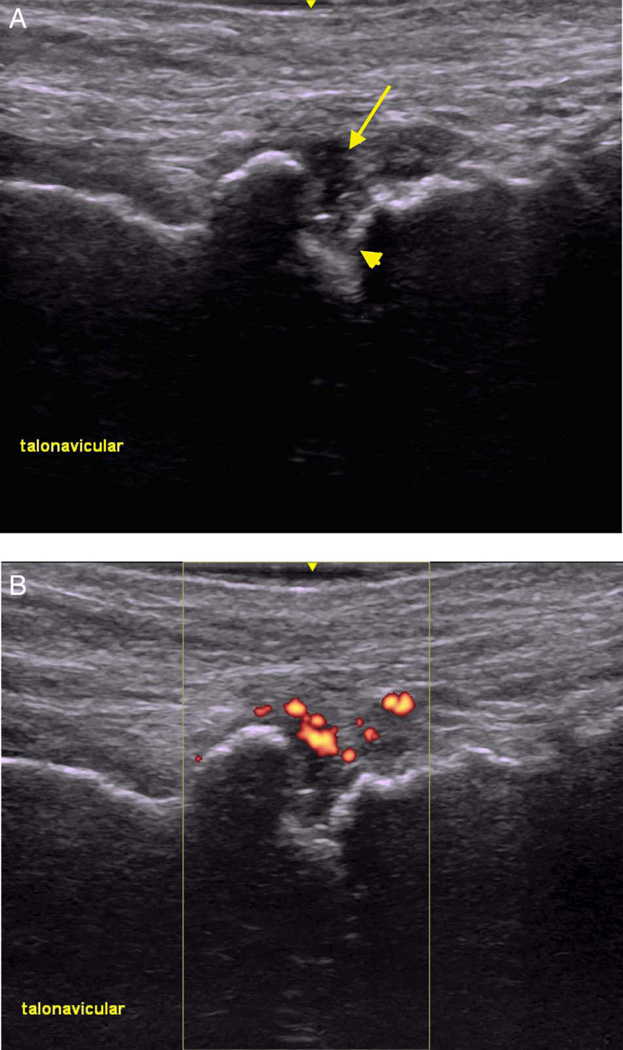
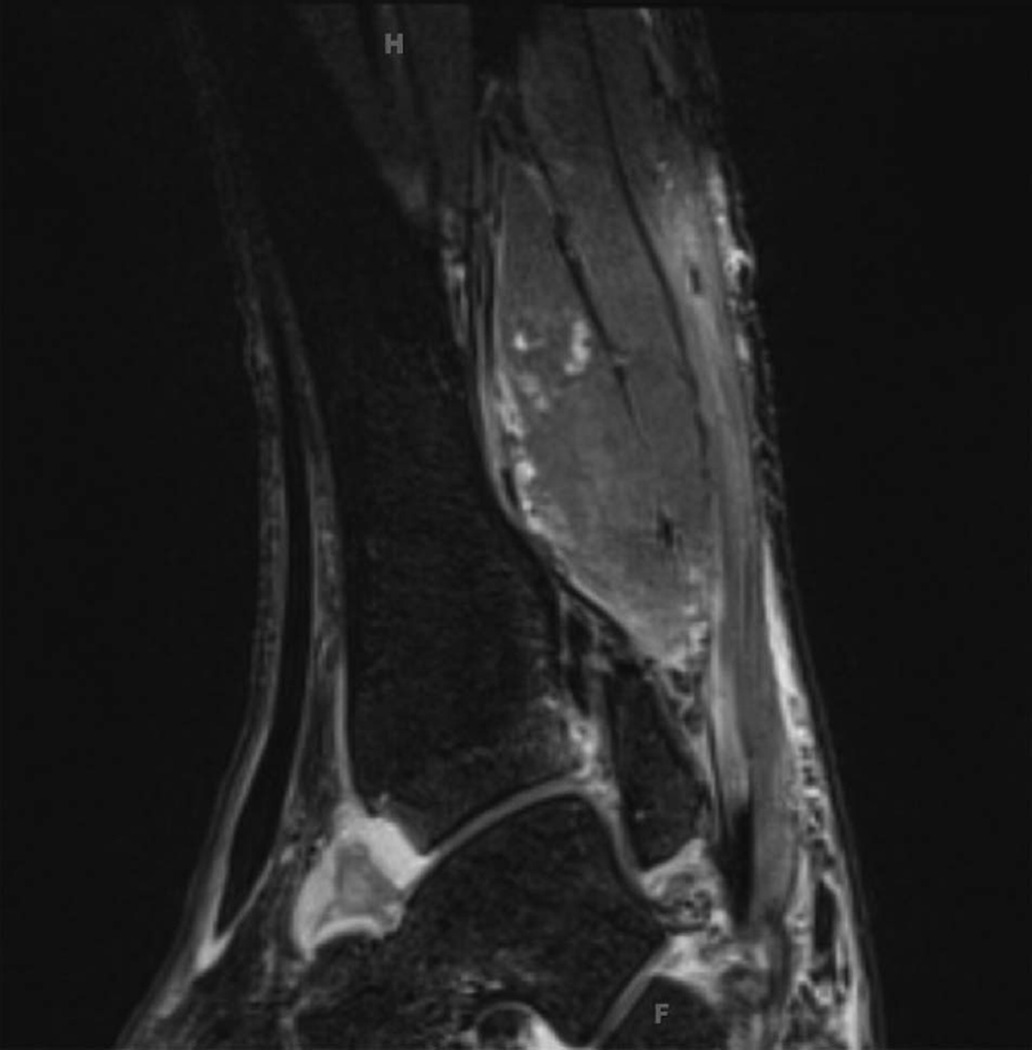
Results: We identified 13 patients who received ICIs and developed rheumatological IRAEs. Mean age was 58.7 years. Cancer types included melanoma, non-small cell lung cancer, small cell lung cancer and renal cell carcinoma. ICI regimens included nivolumab or ipilimumab as monotherapy (n=5), or combination nivolumab and ipilimumab (n=8). Nine of 13 patients developed an inflammatory arthritis, 4 with synovitis confirmed on imaging (3 ultrasound, 1 MRI) and 4 with inflammatory synovial fluid. Four patients developed sicca syndrome with severe salivary hypofunction. Other IRAEs included: pneumonitis, colitis, interstitial nephritis and thyroiditis. Antinuclear antibodies were positive in 5 out of 13 patients. All 13 patients were treated with corticosteroids with varying response. Two patients were treated with methotrexate and antitumor necrosis factor therapy for inflammatory arthritis.
Conclusions: As ICIs are increasingly used for a range of malignancies, new cases of rheumatic IRAEs are likely to emerge. Further research is required to understand mechanisms, determine risk factors and develop management algorithms for rheumatic IRAEs.
Keywords: Arthritis; Autoimmune Diseases; Inflammation; Sjøgren's Syndrome.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Figures
Comment in
-
Checkpoint immunotherapy: good for cancer therapy, bad for rheumatic diseases.Ann Rheum Dis. 2017 Jan;76(1):1-3. doi: 10.1136/annrheumdis-2016-209782. Epub 2016 Aug 26. Ann Rheum Dis. 2017. PMID: 27566797 No abstract available.
References
-
- Lee L, Gupta M, Sahasranaman S. Immune Checkpoint inhibitors: an introduction to the next-generation cancer immunotherapy. J Clin Pharmacol. 2016;56:157–169. - PubMed
-
- Weber JS, D’Angelo SP, Minor D, et al. Nivolumab versus chemotherapy in patients with advanced melanoma who progressed after anti-CTLA-4 treatment (CheckMate 037): a randomised, controlled, open-label, phase 3 trial. Lancet Oncol. 2015;16:375–384. - PubMed
-
- Robert C, Schachter J, Long GV, et al. Pembrolizumab versus ipilimumab in advanced melanoma. N Eng J Med. 2015;372:2521–32. - PubMed
-
- Larkin J, Hodi FS, Wolchok JD. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015;373:1270–1271. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
