

Outcomes With the Use of the Retrograde Approach for Coronary Chronic Total Occlusion Interventions in a Contemporary Multicenter US Registry
- PMID: 27307562
- PMCID: PMC4911894
- DOI: 10.1161/CIRCINTERVENTIONS.115.003434
Outcomes With the Use of the Retrograde Approach for Coronary Chronic Total Occlusion Interventions in a Contemporary Multicenter US Registry
Abstract
Background: We sought to examine the efficacy and safety of chronic total occlusion percutaneous coronary intervention using the retrograde approach.
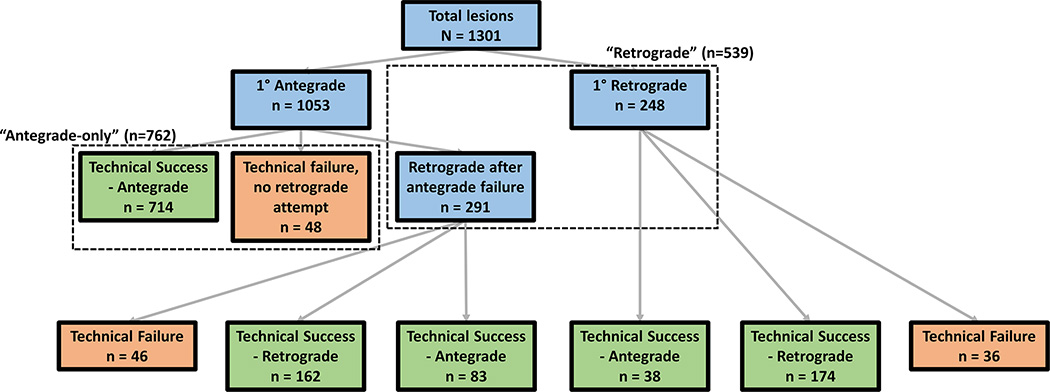
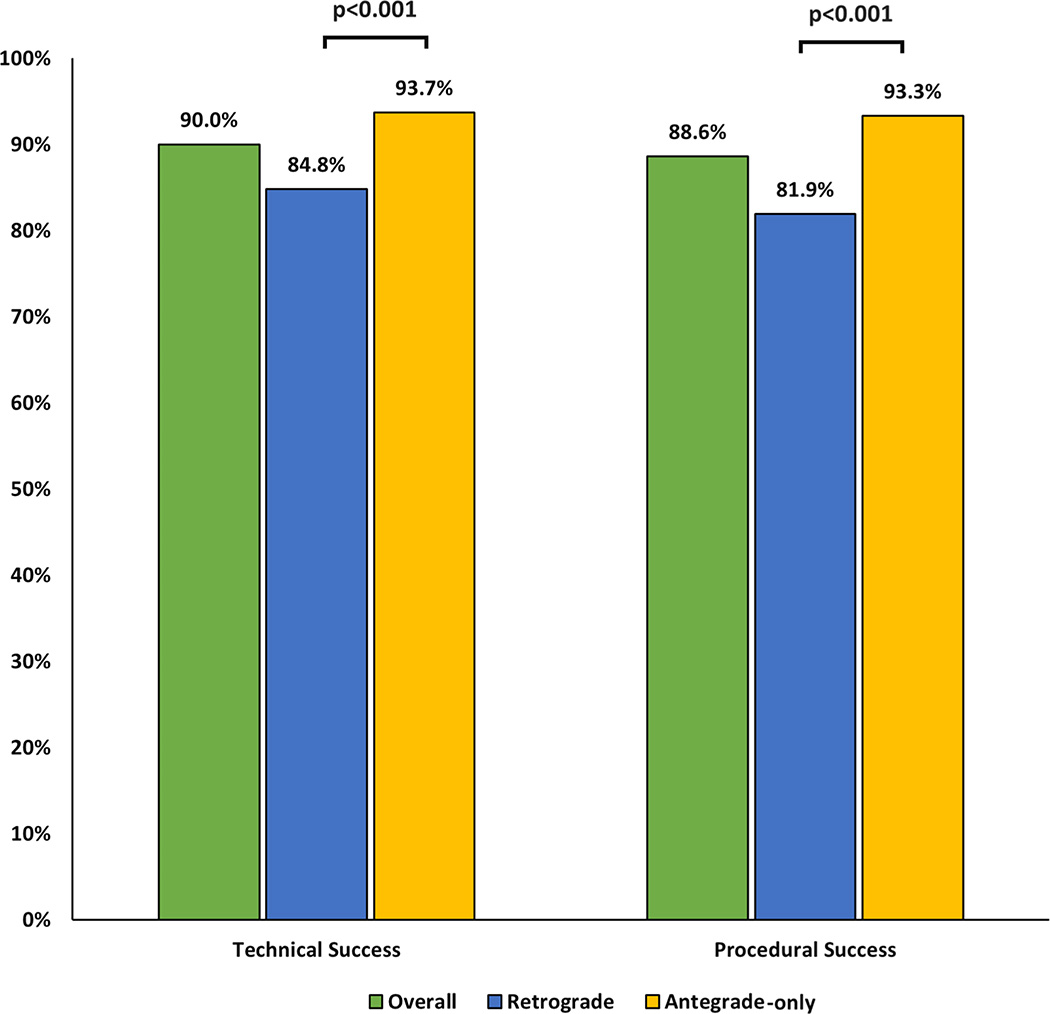
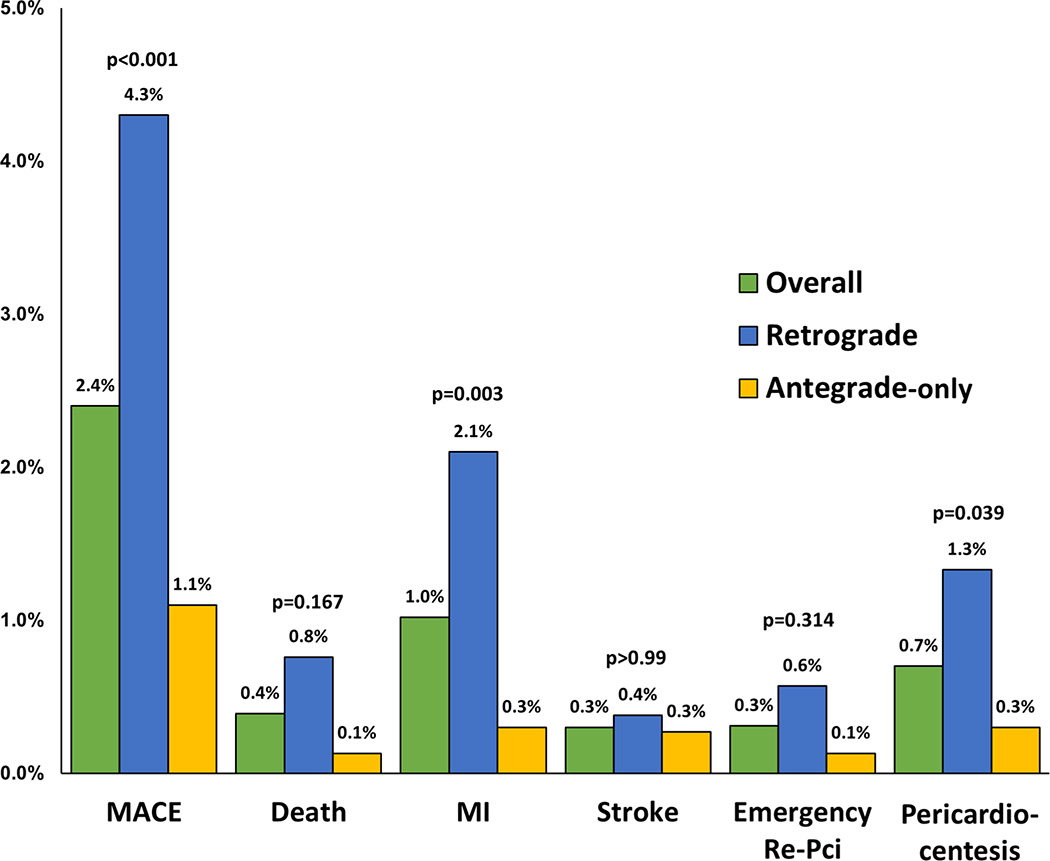
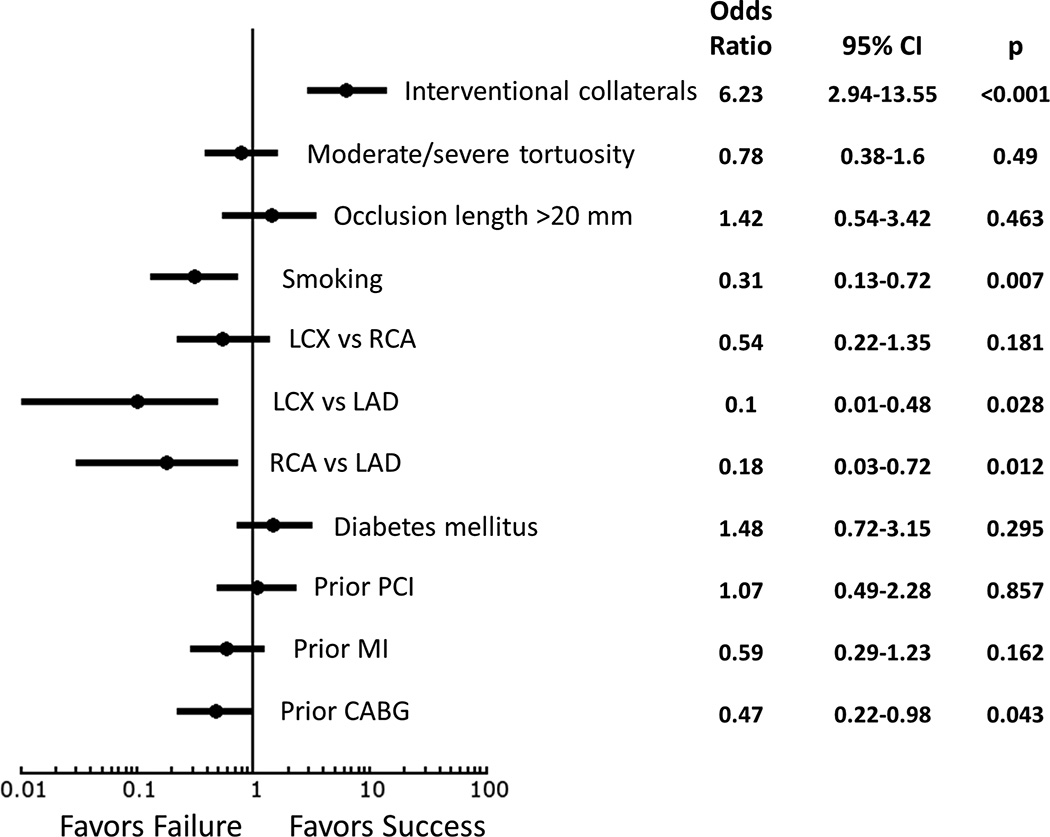
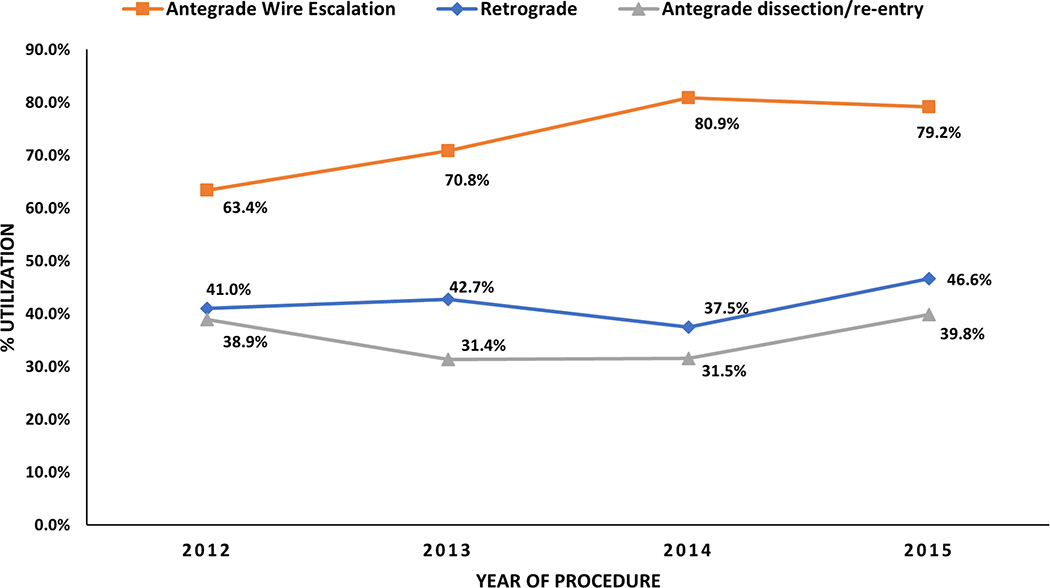
Methods and results: We compared the outcomes of the retrograde versus antegrade-only approach to chronic total occlusion percutaneous coronary intervention among 1301 procedures performed at 11 experienced US centers between 2012 and 2015. The mean age was 65.5±10 years, and 84% of the patients were men with a high prevalence of diabetes mellitus (45%) and previous coronary artery bypass graft surgery (34%). Overall technical and procedural success rates were 90% and 89%, respectively, and in-hospital major adverse cardiovascular events occurred in 31 patients (2.4%). The retrograde approach was used in 539 cases (41%), either as the initial strategy (46%) or after a failed antegrade attempt (54%). When compared with antegrade-only cases, retrograde cases were significantly more complex, both clinically (previous coronary artery bypass graft surgery prevalence, 48% versus 24%; P<0.001) and angiographically (mean Japan-chronic total occlusion score, 3.1±1.0 versus 2.1±1.2; P<0.001) and had lower technical success (85% versus 94%; P<0.001) and higher major adverse cardiovascular events (4.3% versus 1.1%; P<0.001) rates. On multivariable analysis, the presence of suitable collaterals, no smoking, no previous coronary artery bypass graft surgery, and left anterior descending artery target vessel were independently associated with technical success using the retrograde approach.
Conclusions: The retrograde approach is commonly used in contemporary chronic total occlusion percutaneous coronary intervention, especially among more challenging lesions and patients. Although associated with lower success and higher major adverse cardiovascular event rates in comparison to antegrade-only crossing, retrograde percutaneous coronary intervention remains critical for achieving overall high success rates.
Keywords: complication; coronary occlusion; outcome; percutaneous coronary intervention.
© 2016 American Heart Association, Inc.
Figures
Comment in
-
Retrograde Approach for Chronic Total Occlusion Percutaneous Coronary Intervention: The Paradox of Choice.Circ Cardiovasc Interv. 2016 Jun;9(6):e004023. doi: 10.1161/CIRCINTERVENTIONS.116.004023. Circ Cardiovasc Interv. 2016. PMID: 27307563 No abstract available.
References
-
- Rathore S, Matsuo H, Terashima M, Kinoshita Y, Kimura M, Tsuchikane E, Nasu K, Ehara M, Asakura Y, Katoh O, Suzuki T. Procedural and in-hospital outcomes after percutaneous coronary intervention for chronic total occlusions of coronary arteries 2002 to 2008: Impact of novel guidewire techniques. JACC Cardiovasc Interv. 2009;2:489–497. - PubMed
-
- Saito S. Different strategies of retrograde approach in coronary angioplasty for chronic total occlusion. Catheter Cardiovasc Interv. 2008;71:8–19. - PubMed
-
- Surmely JF, Katoh O, Tsuchikane E, Nasu K, Suzuki T. Coronary septal collaterals as an access for the retrograde approach in the percutaneous treatment of coronary chronic total occlusions. Catheter Cardiovasc Interv. 2007;69:826–832. - PubMed
-
- Surmely JF, Tsuchikane E, Katoh O, Nishida Y, Nakayama M, Nakamura S, Oida A, Hattori E, Suzuki T. New concept for cto recanalization using controlled antegrade and retrograde subintimal tracking: The cart technique. J Invasive Cardiol. 2006;18:334–338. - PubMed
-
- Tsuchikane E, Katoh O, Kimura M, Nasu K, Kinoshita Y, Suzuki T. The first clinical experience with a novel catheter for collateral channel tracking in retrograde approach for chronic coronary total occlusions. JACC Cardiovasc Interv. 2010;3:165–171. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
