

Correlation of T2R38 taste phenotype and in vitro biofilm formation from nonpolypoid chronic rhinosinusitis patients
- PMID: 27309535
- PMCID: PMC5500301
- DOI: 10.1002/alr.21803
Correlation of T2R38 taste phenotype and in vitro biofilm formation from nonpolypoid chronic rhinosinusitis patients
Abstract
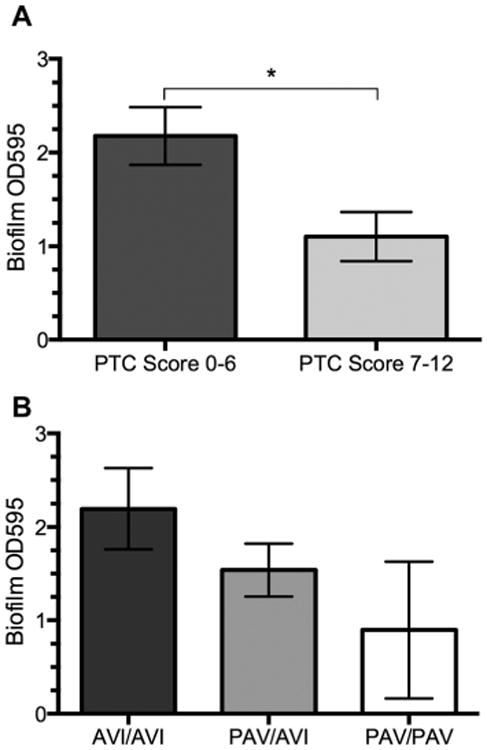
Background: Sinonasal biofilms have been demonstrated in specimens collected from chronic rhinosinusitis (CRS) patients. Mounting evidence suggests that biofilms contribute to therapeutically recalcitrant CRS. Recently, the bitter taste receptor T2R38 has been implicated in the regulation of the sinonasal mucosal innate immune response. TAS2R38 gene polymorphisms affect receptor functionality and contribute to variations seen in sinonasal innate defense as well as taste perception reflected in gustatory sensitivity to the bitter compound phenylthiocarbamide (PTC). In a population of CRS patients with active infection or inflammation, we sought to determine if a correlation between T2R38 phenotype and in vitro biofilm formation existed.
Methods: Endoscopically guided sinonasal swabs were obtained prospectively from CRS (±polyp) patients with evidence of persistent inflammation or mucopurulence. In vitro biofilm formation was assessed with a modified Calgary Biofilm Detection Assay. Patients' phenotypic (functional) expression of the bitter taste receptor T2R38 was evaluated with a taste test including the compound PTC. Linear regression was used to determine the level of significance between mean in vitro biofilm formation levels and mean PTC taste test intensity ratings across CRS patients.
Results: Sinonasal swabs were obtained from 59 patients, with 42 of the 59 samples demonstrating in vitro biofilm formation. Analysis revealed an inverse linear association between in vitro biofilm formation and PTC taste intensity ratings (p = 0.019) for all patients. This association was exclusively driven by nonpolypoid CRS patients (p = 0.0026).
Conclusion: In vitro biofilm formation from sinonasal clinical isolates is inversely correlated with PTC taste sensitivity in nonpolypoid CRS patients.
Keywords: Calgary biofilm detection; Pseudomonas aeruginosa; T2R38 polymorphism; biofilm; bitter taste receptor; chronic rhinosinusitis; genetics; nitric oxide; phenylthiocarbamide; supertaster.
© 2016 ARS-AAOA, LLC.
Conflict of interest statement
Potential conflict of interest: N.A.C. has a patent pending “Therapy and Diagnostics for Respiratory Infection.”
Figures



References
-
- Bhattacharyya N, Grebner J, Martinson NG. Recurrent acute rhinosinusitis: epidemiology and health care cost burden. Otolaryngol Head Neck Surg. 2012;146:307–312. - PubMed
-
- Bhattacharyya N. Incremental healthcare utilization and expenditures for allergic rhinitis in the United States. Laryngoscope. 2011;121:1830–1833. - PubMed
-
- Khalid AN, Quraishi SA, Kennedy DW. Long-term quality of life measures after functional endoscopic sinus surgery. Am J Rhinol. 2004;18:131–136. - PubMed
-
- Simopoulos E, Katotomichelakis M, Gouveris H, Tripsianis G, Livaditis M, Danielides V. Olfaction-associated quality of life in chronic rhinosinusitis: adaptation and validation of an olfaction-specific questionnaire. Laryngoscope. 2012;122:1450–1454. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
